Tadalafil entfaltet seine Wirkung über eine selektive Hemmung der PDE5, wodurch die Konzentration von cGMP im glatten Muskelgewebe stabil bleibt. Diese biochemische Modulation resultiert in einer langanhaltenden Relaxation der Gefäßwände. Der Wirkstoff wird nach oraler Einnahme effizient resorbiert, mit einer Bioverfügbarkeit von rund 80 %. Seine Halbwertszeit von bis zu 36 Stunden ist innerhalb dieser Substanzklasse außergewöhnlich. Abgebaut wird er in der Leber, hauptsächlich durch CYP3A4, mit anschließender biliärer Exkretion. Typische unerwünschte Wirkungen entstehen durch eine verstärkte Vasodilatation, etwa Kopfschmerzen oder Flush. Pharmakologisch wird cialis generika vor allem durch die verlängerte Wirkungsdauer charakterisiert.
Doi:10.1016/j.jcrs.2005.11.015
J CATARACT REFRACT SURG - VOL 32, JANUARY 2006
Transient light sensitivity after femtosecond laser
flap creation: Clinical findings and management
Karl G. Stonecipher, MD, Jon G. Dishler, MD, Teresa S. Ignacio, MD, Perry S. Binder, MD
PURPOSE: To describe the constellation of subjective and objective findings associated with unusualoccurrences of photosensitivity after laser in situ keratomileusis (LASIK) with femtosecond flap creationand identify optimal management strategies.
METHODS: Demographic data, laser settings, subjective complaints, clinical findings, treatment, andresponse to treatment were recorded for suspected cases of transient postoperative photosensitivityfrom 3 surgeons operating at 3 different sites. All cases were estimated for the period covering thesuspected cases at each site to assess incidence. Additional cases were solicited from IntraLase usersvia a survey.
RESULTS: For the 3 sites, 63 eyes from 33 patients were reported of a total estimated case log of 5667(incidence, 1.1%). Average age was 41 years, and 51.7% of patients were women. Onset of symptomsranged from 2 to 6 weeks after uneventful LASIK. All patients were treated with prednisolone acetatedrops, whereas 1 surgeon also used Restasis (cyclosporine ophthalmic solution 0.05%). Patients notedimprovement of symptoms within 1 week of treatment. When the raster and side-cut energy settingswere lowered (by an average of 24% and 33%, respectively), significant reductions in incidence werenoted. Similar findings were reported by 3 additional surgeons reporting 17 cases in the survey ofIntraLase users.
CONCLUSIONS: This report describes a new complication of LASIK performed with a femtosecondlaser keratome that may be related to the pulse energy used for flap creation. Although there is noloss of uncorrected visual acuity, symptoms can be prolonged, especially without prompt steroid ther-apy. Technical advances that reduced pulse energies appear to decrease the incidence.
J Cataract Refract Surg 2006; 32:91–94 Q 2006 ASCRS and ESCRS
The mechanism of femtosecond laser flap creation with the
been reported to reduce or eliminate many of the minor
IntraLase FS (IntraLase Corp.) has been described exten-
and severe complications associated with flap
sively.Briefly, the system produces short-duration (600
More recently, sporadic cases of unusual photosensitiv-
to 800 femtosecond) light pulses at 1053 nm infrared wave-
ity that does not affect visual acuity have been reported (B.
length. Multiple pulses are focused to an approximately
Will, MD, ‘‘Success with IntraLase: It’s Not Just Point and
3 mm spot diameter at a preset depth, leading to photo-
Shoot’’; K. Stonecipher, MD, ‘‘A Comparative Study: Moria,
disruption and creation of a corneal resection plane.
Hansatome, and Intralase’’; both presented at the ASCRS
Once the bed of the flap has been created, the device cre-
Symposium on Cataract, IOL and Refractive Surgery, San
ates a side cut from the level of the resection plane, mov-
Diego, California, USA, May 2004). The term transient light
ing anteriorly through the epithelium. Cavitation bubbles
sensitivity syndrome (TLSS) has been coined to describe this
created during photodisruption generally remain in the
condition. A multicenter case series is reported to describe
resection plane; however, they may migrate anteriorly,
the constellation of subjective and objective findings as
posteriorly, or peripherally in the cornea.
well as clinical outcomes seen with this entity.
Initial experience in the United States with the Intra-
Lase FS laser began in May 2000 and showed excellent
results with no postoperative complicTo date,
Suspected postoperative photosensitivity cases were divided
several studies have documented improved flap predict-
into 3 groups according to the surgeon reporting them ().
ability and refractive outcomes compared with that of the
For each group, demographic data, reported symptoms,
mechanical microkeratome.Use of the technology has
uncorrected visual acuity (UCVA), slitlamp examination, and
Table 1. Summary of suspected postoperative photosensitivity cases
20/20 to 20/30). Slitlamp examination found no internal or
grouped according to reporting surgeon.
external inflammatory reaction and no significant interfacefindings. Patients were treated with prednisolone acetate
1% (Pred Forte) as frequently as hourly or 4 times per
day for 1 to 2 weeks. The Pred Forte was tapered after
1 week or over 1 to 2 months. Symptoms resolved within
1 to 2 weeks of topical steroid therapy, with no change in
*Although only 6 cases were reported with clinical data, approximately
20 cases were suspected in retrospect before recognition of the entity.
After the laser bed energy settings were lowered to
2.3 mJ (39% decrease) and side-cut energy to 3.2 mJ (64%decrease), no additional similar cases were reported. In
response to interventions were recorded from clinical records. Raster and side-cut energy used for femtosecond laser flap crea-
addition to these laser setting changes, the postoperative
tion were also recorded. Estimates of incidence rates were made
medication regimen was changed from loteprednol 0.5%
based on the number of procedures performed during the relevant
eyedrops (Lotemax) 4 times a day for 1 week to Pred Forte
time interval at each respective clinical site.
Additional cases were collected from a survey distributed to
all IntraLase users, which solicited data on suspected TLSS casesincluding patient symptoms, clinical findings, demographics, la-
ser energy settings, and treatment; responses were received be-tween August and November 2004.
Thirty-two eyes of 16 patients reporting severe light
sensitivity were collected from a cohort of 2994 eyes (inci-dence of 1.06%) having LASIK between January 2003 and
September 2004. The mean patient age was 41 years (range
25 to 57 years) and the mean preoperative spherical equiv-alent was ÿ4.6 diopters (D) (range ÿ0.9 to ÿ8.75 D) and
the mean cylinder, 0.94 D (range 0.0 to 2.5 D). Sixty per-
Eleven eyes of 6 patients were identified from a cohort
cent of the patients were women. The iris color was brown
of 783 cases followed up prospectively in 2001. Approxi-
in 37.5% (12 of 32), blue in 37.5% (12 of 32), and hazel in
mately 14 additional patients may have experienced similar
25% (8 of 32). Preoperative UCVA ranged from 20/200 to
symptoms but were not specifically identified, so their
counting fingers. The mean preoperative best corrected
data were not available for review. The mean age of affected
visual acuity (BCVA) was 1.01 G 0.08 (range 0.8 to
patients was 43 years (range 37 to 47 years), and 50% were
1.33). The mean postoperative UCVA was 1.03 G 0.19
women. Patients presented with complaints of extreme sen-
(range 0.5 to 1.33). One eye of 1 patient with a visual acuity
sitivity to indoor lights and computer screens. The onset of
of 20/200 was planned for monovision, with the other
symptoms ranged between 3 and 6 weeks after uneventful
96.5% having 20/25 or better. The mean postoperative
laser in situ keratomileusis (LASIK). The mean laser bed
BCVA was 1.11 G 0.16 (range 1.33 to 1.0), with 100% of
(raster) energy was 3.75 mJ G 1.3 (SD), and the mean side-
the population correctable to 20/20 or better. The mean
cut energy was 8.75 G 0.12 mJ. The mean UCVA (decimal)
preoperative pachymetry was 542.5 G 24.4 mm. The mean
at the time of reported symptoms was of 0.95 G 0.1 (range
photopic pupil size was 4.63 G 1.02 mm (range 3.0to 6.6 mm) and the mean scotopic pupil size, 6.13 G0.74 mm (range 5 to 7 mm). There were no perioperative
Accepted for publication April 8, 2005.
From the Southeastern Laser and Refractive Center (Stonecipher),
Onset of photophobia occurred between 4 and 6 weeks
Greensboro, North Carolina; Dishler Laser Institute (Dishler),
postoperatively with normal visual acuity at the time of com-
Denver, Colorado; the Department of Ophthalmology (Ignacio),
plaint. The mean raster energy used was 3.4 G 0.5 mJ and
University of California Irvine, California; and Gordon Binder and
the mean side-cut energy, 4.3 G 0.89 mJ. On slitlamp exam-
Weiss Vision Institute (Binder), San Diego, California, USA.
ination, anterior segments in all patients were normal with
Dr. Stonecipher and Dr. Dishler have received travel and research
no significant detectable interface inflammation or deposits.
support from IntraLase. Dr. Binder and Dr. Ignacio are consultantsto IntraLase Corp.
Patients were given Pred Forte 4 to 6 times a day or Restasis(cyclosporine ophthalmic solution 0.05%) 2 to 4 times per
No author has a financial or proprietary interest in any material ormethod mentioned.
day for the first week or 2 after presentation, and improve-ment of symptoms was noted after a week of treatment.
Reprint requests to Perry S. Binder, MD, Gordon Binder Vision In-stitute 8910 University Center Lane, Suite 800, San Diego Califor-
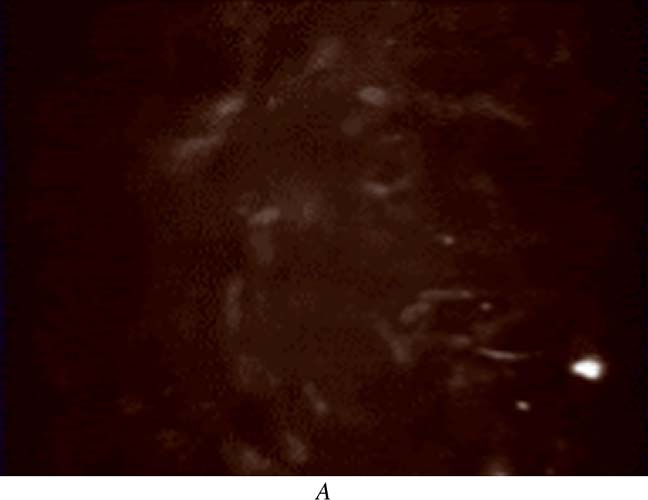
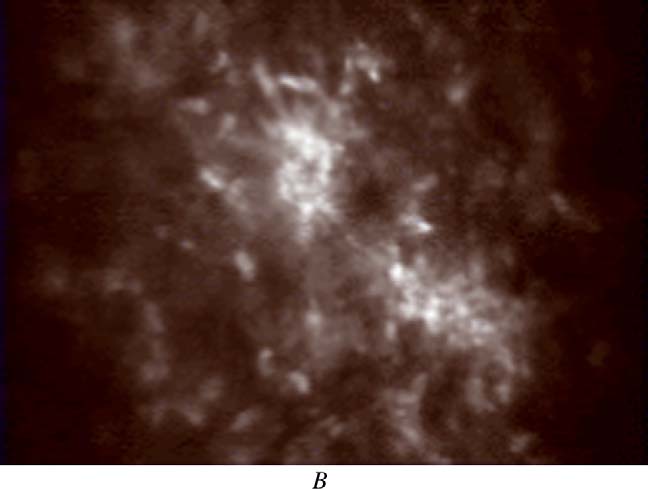
Confocal imaging was performed in some eyes and
compared with asymptomatic cases (). Findings
J CATARACT REFRACT SURG - VOL 32, JANUARY 2006
had planned monovision with 20/200 and 20/300 in eacheye. All remaining eyes had acuities of 20/30 or better. Onslitlamp examination, no signs of inflammation were notedin any eye. Patients were treated with hourly drops of PredForte for 7 days. All patients responded to treatment, andthere were no chronic cases seen. Laser side-cut energysetting was lowered subsequently to 3.6 mJ (decreased by10%). Incidence of this entity was 1% (5 of 500) after thedecrease in laser energy settings.
In the survey, an additional 17 eyes of 10 patients were
reported by 3 surgeons from different clinical sites. Allpatients were women with a mean age of 47 years (range26 to 63 years). Patients’ complaints were light sensitivityand glare. The mean raster energy used was 1.97 G 0.3 mJ(range 1.8 to 2.5 mJ), and the mean side-cut energy was3.42 G 0.3 mJ (range 3 to 3.6 mJ). The mean UCVA was0.90 G 0.3 (range 20/20 to 20/80). One eye of 1 patienthad an acuity of 20/150 after planned monovision treat-ment. On slitlamp examination, 4 eyes showed mild inter-face haze. However, the same interface haze was seen inother patients who did not complain of light sensitivity. Treatment varied according to surgeon preference. Medica-tion regimens included Lotemax 0.5% eyedrops 4 timesa day for 2 weeks and prednisolone acetate ophthalmic sus-pension (Econopred 1ˇ/8%) twice a day for 2 weeks. Symp-toms began to resolve after 1 week of treatment in allcases, and no loss of BCVA was reported in any case.
Laser energy settings used by surgeons and surgeons
who participated in the survey are summarized in
Figure 1. A: Confocal image of a post-LASIK interface of an asymptomaticpatient. B: Confocal image of a stromal interface in a patient with TLSS.
Probable activated keratocytes are present.
Transient light sensitivity syndrome describes a con-
stellation of symptoms that can occur after LASIK with fem-
included activated keratocytes at the interface that resolved
tosecond laser flap creation. Patients with TLSS generally
with the resolution of the patient’s subjective complaints.
present with light sensitivity that is out of the ordinary,
Laser bed energy and side-cut energy were reduced subse-
good UCVA, and minimal slitlamp findings 2 to 6 weeks af-
quently by 20.5% to 2.7 mJ and 25.7% to 3.2 mJ, respectively.
ter uneventful LASIK. All patients responded to topical ste-
Incidence of TLSS was reduced to 0.17% (3 of 1705) after
roids, although improvement with Restasis has also been
the decrease in laser energy settings.
reported by 1 center. Based on collected cases, an incidenceof approximately 1% was identified. The highest incidence
rates occurred with the highest initial energy settings and
Twenty eyes of 11 patients were collected from a cohort
with reduction in the number of cases after reductions in
of 1900 patients having LASIK between August 2003 and
laser energy settings by 20% to 60%. In best documented se-
August 2004 (incidence 1.05%). The mean age was 39 years
ries (group 2), there was an approximately 5-fold reduction
(range 26 to 56 years), and 45% of the patients were women.
in incidence to less than 0.2% after an approximately 20%
Patients presented 2 to 6 weeks after surgery with sensitivity
to room light severe enough to make them unable to watch
The etiology of this syndrome is unknown, but the
television or use the computer. The mean laser bed energy
identification of activated keratocytes at the interface that
was 1.98 G 0.17 mJ, and the mean and side-cut energy
in some cases resolve with the resolution of the patient’s
was 4.0 mJ. The mean UCVA was 0.89 G 0.27. Two patients
subjective complaints is noteworthy. However, these cells
J CATARACT REFRACT SURG - VOL 32, JANUARY 2006
Table 2. Summary of laser energy settings used by different surgeons.
are also seen in patients with no symptoms. Activated
low incidence of the entity seen after reduction in laser
keratocytes are a feature of normal healing after LASIK,
energy settings may make this impractical. Animal studies
and they have been reported to occur after other refractive
may therefore provide additional information regarding
procedures as well. The reduction in TLSS cases after laser
this phenomenon. Technical advances in the device that
energy settings were lowered supports secondary effects of
permit even lower energy settings may also help reduce
laser pulse energy, such as shock wave exposure on local
keratocytes or corneal nerve endings, as an etiology. Reduc-tion in laser energy reduces the magnitude and range ofthese transients, thereby possibly reducing their effects
on local cell populations. Similar symptoms have beenreported more rarely after LASIK performed with a mechan-
1. Kurtz RM, Liu X, Elner VM, et al. Photodisruption in the human cornea
as a function of laser pulse width. J Refract Surg 1997; 13:653–658
2. Sugar A. Ultrafast (femtosecond) laser refractive surgery. Curr Opin
tion may occur via different mechanisms as well. Another
etiology may be associated with migration of the expelled
3. Ratkay-Traub I, Juhasz T, Horvath C, et al. Ultra-short pulse (femtosec-
gases into the peripheral cornea and episclera that could
ond) laser surgery; initial use in LASIK flap creation. Ophthalmol Clin
irritate the ciliary body. Because the eyes respond to topical
steroids, some irritation of the ciliary body can be
4. Nordan LT, Slade SG, Baker RN, et al. Femtosecond laser flap creation
for laser in situ keratomileusis: six-month follow-up of initial US clinical
Although no definite etiologic mechanism has been
5. Ratkay-Traub I, Ferincz IE, Juhasz T, et al. First clinical results with the
identified, several management strategies can be recom-
femtosecond neodynium-glass laser in refractive surgery. J Refract
mended based on the summarized clinical experience to
reduce incidence and severity of TLSS. These include:
6. Kezirian GM, Stonecipher KG. Comparison of the IntraLase femtosec-
ond laser and mechanical keratomes for laser in situ keratomileusis.
1. The lowest possible surgical energy settings needed
J Cataract Refract Surg 2004; 30:804–811
to maintain good flap dissection quality should be
7. Binder PS. Flap dimensions created with the IntraLase FS laser. J Cat-
used, usually combined with reduction in laser
8. Tran DB, Sarayba MA, Bor Z, et al. Randomized prospective clinical
spot separations to allow lower energy settings.
study comparing induced aberrations to IntraLase and Hansatome
2. Patients presenting with photosensitivity should be
flap creation in fellow eyes: potential impact on wavefront-guided
examined for evidence of true diffuse lamellar
laser in situ keratomileusis. J Cataract Refract Surg 2005; 31:97–105
keratitis.If available, confocal microscopy may
9. Anderson NJ, Edelhauser HF, Sharara N, et al. Histologic and ultrastruc-
tural findings in human corneas after successful laser in situ keratomi-
be considered for additional information directing
leusis. Arch Ophthalmol 2002; 120:288–293
treatment. Eyes can be treated with prednisolone
10. Kramer TR, Chuckpaiwong V, Dawson DG, et al. Pathologic findings in
acetate 1% every 1 to 6 hours tapered over 1 to 4
postmortem corneas after successful laser in situ keratomileusis.
weeks. Patients should be monitored for evidence
of elevated intraocular pressure. Adjunctive use
11. Lackner B, Pieh S, Schmidinger G. Glare and halo phenomena after
laser in situ keratomileusis. J Cataract Refract Surg 2003; 29:444–450
of nonsteroidal antiinflammatory medications can
12. Jabbur NS, Sakatani K, O’Brien TP. Survey of complications and re-
also be considered (Frank Price, MD, personal
commendations for management in dissatisfied patients seeking a
consultation after refractive surgery. J Cataract Refract Surg 2004;30:1867–1874
Further clinical studies may help identify more specific
13. Linebarger EJ, Hardten DR, Lindstrom RL. Diffuse lamellar keratitis: di-
etiologies and management of TLSS. However, the relatively
agnosis and management. J Cataract Refract Surg 2000; 26:1072–1077
J CATARACT REFRACT SURG - VOL 32, JANUARY 2006
N'Aleminum-Gusta Det finns många män och kvinnor av betydelse i vår långa historia som aldrig fått ett erkännande av sin samtid. Det är med en viss inre tillfredsställelse jag här och nu vill ge några rader ur minnet av en av dessa gestalter i min hemby under 20-30 talet och framåt. Hans namn var Gustav Jonsson född 27/12-1870 och dog den 1/12-1955. Denne särpräglade och unike le
Why buy expensive Aloe vera soothing products for stings, cuts, abrasions and skin problems etc when you can make your own for free ? It is so easy to do. All you need, really, is an Aloe vera plant – and we can supply you with that. Simply go to the Health and Wellbeing section of our shop at www.wikaniko.com and get your very own Aloe vera plant! The next thing you need to do is sim
 had planned monovision with 20/200 and 20/300 in eacheye. All remaining eyes had acuities of 20/30 or better. Onslitlamp examination, no signs of inflammation were notedin any eye. Patients were treated with hourly drops of PredForte for 7 days. All patients responded to treatment, andthere were no chronic cases seen. Laser side-cut energysetting was lowered subsequently to 3.6 mJ (decreased by10%). Incidence of this entity was 1% (5 of 500) after thedecrease in laser energy settings.
had planned monovision with 20/200 and 20/300 in eacheye. All remaining eyes had acuities of 20/30 or better. Onslitlamp examination, no signs of inflammation were notedin any eye. Patients were treated with hourly drops of PredForte for 7 days. All patients responded to treatment, andthere were no chronic cases seen. Laser side-cut energysetting was lowered subsequently to 3.6 mJ (decreased by10%). Incidence of this entity was 1% (5 of 500) after thedecrease in laser energy settings.