Tadalafil entfaltet seine Wirkung über eine selektive Hemmung der PDE5, wodurch die Konzentration von cGMP im glatten Muskelgewebe stabil bleibt. Diese biochemische Modulation resultiert in einer langanhaltenden Relaxation der Gefäßwände. Der Wirkstoff wird nach oraler Einnahme effizient resorbiert, mit einer Bioverfügbarkeit von rund 80 %. Seine Halbwertszeit von bis zu 36 Stunden ist innerhalb dieser Substanzklasse außergewöhnlich. Abgebaut wird er in der Leber, hauptsächlich durch CYP3A4, mit anschließender biliärer Exkretion. Typische unerwünschte Wirkungen entstehen durch eine verstärkte Vasodilatation, etwa Kopfschmerzen oder Flush. Pharmakologisch wird cialis generika vor allem durch die verlängerte Wirkungsdauer charakterisiert.
Akademikpersonel.kocaeli.edu.tr
Short Communication
Characteristics of the Turkish Isolates of Francisella tularensis
¸aban Gürcan*, O˘guz Karabay1, Aynur Karadenizli2, Çi˘gdem Karagöl,
Trakya University, Faculty of Medicine, Department of Microbiology and Clinical Microbiology, Edirne;1˙Izzet Baysal University, Faculty of Medicine, Department of Infectious Diseases andClinical Microbiology, Bolu; 2Kocaeli University, Faculty of Medicine, Department of Microbiology andClinical Microbiology, Kocaeli, Turkey; and 3National Center of Infectious and Parasitic Diseases,Department of Microbiology, Sofia, Bulgaria
(Received November 12, 2007. Accepted March 12, 2008)
SUMMARY: In this study, cultures of patients with tularemia were evaluated, and antimicrobial susceptibilities of two Francisella tularensis strains were tested by disk diffusion and E-test methods. A high-resolution multiple- locus variable-number tandem repeat analysis (MLVA) comprising six variable-number tandem repeat loci was applied to elucidate the genetic relatedness among Turkish and Bulgarian isolates which were isolated in a recent outbreak. The patients were diagnosed in two outbreaks in two cities of Turkey in 2005 and 2006. A total of 16 samples from 12 patients were cultured, and PCR tests were carried out on 15 samples that were positive in five lymph node aspirates and two soft tissue aspirates. F. tularensis was isolated from the lymph nodes of two patients. Aminoglycosides, quinolones, chloramphenicole, tetracyclines, nitrofurantoin, and rifampicin inhibited growth of the isolates. The Turkish isolates appeared to share a common MLVA pattern with one of the four Bulgarian outbreak genotypes.
In recent years, tularemia outbreaks have been reported
cystine, 1% glucose and 5% human blood in the presence or
from some regions in Turkey (1). According to data of 2005,
absence of 1,000 U/ml penicillin. If the bacteria were small,
431 confirmed tularemia cases were reported from 19 cities
pale-staining, Gram-negative coccobacilli, without hemoly-
of Turkey in 2005 (2). Oropharyngeal tularemia is the main
sis, weakly catalase positive, as well as oxidase negative, they
clinical form, and only one fatal case has been reported in
were considered probable isolates of F. tularensis. Subse-
Turkey (1). These data predict that Francisellatularensis
quently, they were identified as F. tularensis by TaqMan PCR
subsp. holarctica may be a dominant subspecies in Turkey,
but this hypothesis had not been confirmed yet.
The antibiotic-free media for the culture defined above were
In this study, cultures of patients with tularemia were evalu-
used for the susceptibility tests. Bacteria were grown for 48 h
ated, polymerase chain reaction (PCR) testing was applied
at 37°C in atmospheric air, and the colonies were suspended
to these samples and antimicrobial susceptibilities of two F.
in saline to achieve a turbidity equivalent to that of McFarland
tularensis were tested by disk diffusion and the E-test meth-
standard 1. The plates were inoculated with 100 l of a colony
od. Additionally, a high-resolution multiple-locus variable-
suspension. Ten to 15 min later, E-test strips (AB Biodisk,
number tandem repeat analysis (MLVA) was applied to eluci-
Solna, Sweden) and antibiotic disks (Becton Dickinson) were
date the genetic relatedness among Turkish and Bulgarian
placed on the plates with proper distancing among them.
isolates. The patients were diagnosed during outbreaks in two
Minimum inhibitory concentrations (MICs) and zone diam-
cities of Turkey in 2005 and 2006 (1). In clinically compatible
eters were read after 48 h of incubation at 37°C in atmos-
cases, a microagglutination test was performed on a V plate
(1). BD Francisella tularensis antigen (Becton Dickinson,
The isolation and characterization of Bulgarian isolates are
Sparks, Md., USA) was used in the microagglutination tests
described elsewhere (5). A high-resolution MLVA typing
for the initial diagnosis. Two in-house antigens were prepared
system comprising six variable number of tandem repeats
from the two F. tularensis isolates cultured in the present
(VNTR) loci was applied to the Turkish and Bulgarian iso-
study, as previously described (3). The test results, which were
lates. Some modifications were made to the MLVA protocol
repeated by in-house antigens, were identical with results of
described by Byström et al. (6). For compatibility with
ALFexpressII sequencer (GE Healthcare Life Sciences,
A total of 16 samples from 12 patients from villages of the
Piscataway, N.J., USA) the Ft-M3, Ft-M6, Ft-M20, Ft-M21,
Thrace region and the western Black Sea region of Turkey
Ft-M22, and Ft-M24 primers were labeled with Cy5 instead
were studied. Clinical samples were obtained by a suitable
of 6-carboxytetramethylrhodamine (6,7). The primer concen-
technique. PCR assays were performed as described elsewhere
trations were adjusted as follows: Ft-M3 - 0.12
(4) in all samples except one lymph node aspirate sample.
M6 - 0.15 M, Ft-M20 - 0.05 M, Ft-M21 - 0.06 M, Ft-
All samples were cultured on agar supplemented with 0.1%
M22 - 0.03 M, and Ft-M24 - 0.5 M. The reaction volumewas 25 l with the following concentrations of PCR com-
*Corresponding author: Mailing address: Trakya University, Fac-
ulty of Medicine, Department of Microbiology and Clinical
(50 mM KCl, 20 mM Tris-HCl, pH 8.4, Invitrogen Corp.,
Microbiology, 22030-Edirne, Turkey. Tel & Fax: +90-284-2361654,
Carlsbad, Calif., USA), 5% DMSO (Merck KGaA, Darmstadt,
Germany), 0.1 g/ l non-acetylated bovine serum albumin
(Sigma-Aldrich, St. Louis, Mo., USA), 1 U Taq polymerase
presented with a single allele. The two Turkish isolates were
(Invitrogen). The cycling program was as described by
found to be identical to each other, as well as to one of the
Johansson et al. (7). Three microliters of PCR products was
Bulgarian outbreak clusters (Fig. 1).
mixed with an equal volume of loading buffer (99.5% deion-
Oropharyngeal tularemia is the most common clinical form
ized formamide, 0.5% blue dextran), denatured for 5 min at
of the disease, because almost all tularemia outbreaks are
94°C and loaded on an 8% ReproGel (GE Healthcare Life
water-borne diseases in the Balkans and Anatolia (1). F.
Sciences). Separation was performed on an ALFexpressII
tularensis enters the human body via the consumption of con-
DNA sequencer (GE Healthcare Life Sciences). Electrophore-
taminated water or food in oropharyngeal form. F. tularensis
sis conditions were according to the manufacturer’s instruc-
or its DNA were demonstrated in water specimens in Turkey
tions. The gel processing and cluster analysis of the MLVA
(1). Although one of 12 patients with oropharyngeal tularemia
patterns were performed in Bionumerics v4.5 (Applied Maths
in the present study had neurological symptoms (fever and
NV, Kortrijk, Belgium) software. A dendrogram was gener-
headache), the possibility of central nervous system infec-
ated using categorical coefficient and unweighted pair-group
tion was eliminated in this case by CSF assays.
with arithmetic means (UPGMA) algorithms.
Since the confirmation of tularemia by culture is generally
All patients’ antibodies against F. tularensis were positive
unsuccessful, this disease is often diagnosed with serological
in 1/160 - 1/5,120 dilutions. Out of 16 samples, nine were lymph
tests and molecular methods as well as clinical findings in
node aspirates, three were throat swabs, two were aspirates
Turkey and other parts of the world. Our cases were diag-
from the soft tissue of the cheek, one was an oral lesion swab
nosed within 8 weeks after the onset of symptoms by sero-
and one was cerebrospidal fluid (CSF). Two F. tularensis
logical tests. In the present study, the fact that 7 of 15 samples
isolates were isolated from the lymph node aspirates of two
were positive emphasizes the importance of molecular biol-
patients living in the western Black Sea region in December
ogy techniques for the early diagnosis of tularemia.
2005. PCR tests were positive in five lymph node aspirate
Clinicians in Turkey have little experience in the use of
samples and two soft tissue aspirates. Susceptibility zones
culturing for the routine diagnosis of tularemia due to the high
for these isolates were determined for aminoglycosides,
degree virulence of the organism, the high risk of laboratory-
quinolones, tetracyclines, chloramphenicol, nitrofurantoin, and
acquired infection and the low sensitivity of the culture. F.
rifampicin by disk diffusion and E-tests, but no zone was seen
tularensis was isolated in 10 (4.9%) out of 205 patients be-
around beta-lactam antibiotics, erythromycin or co-trimoxazole
tween 1988 and 1998 in Turkey (1). In the present study, two
isolates were isolated from the lymph node aspirates of two
A total of four genotypes were found among the nine in-
patients living in the western Black Sea region of Turkey.
vestigated isolates (7 Bulgarian and 2 Turkish) (Fig. 1). The
The Black Sea region is where most of the tularemia cases
M3 marker appeared to be the most variable one, showing
are reported in Turkey (1). There has been no isolation of F.
four different alleles among the nine isolates studied, followed
tularensis isolates and no data collected regarding the anti-
by M6 (3 alleles) and M20 (2 alleles). All other markers were
microbial susceptibilities of F. tularensis isolates from the
Table 1. Susceptibilities of antimicrobials for two Turkish isolates of Francisella tularensis by
Penicillin, SAM, AMC, Piperacillin, PTZ, Oxacillin
1): Yazikara strains. 2): Nuhoren strains. SAM, Ampicillin/sulbactam; AMC, Amoxicillin/clavulanate; PTZ, Piperacillin/tazobactam; NZ, nozone; ND, not determined.
Fig. 1. MLVA cluster analysis of Bulgarian and Turkish Francisella tularensis strains comprising six VNTR loci (M3 to
M24). The corresponding fragment sizes (in base pairs) are given below each VNTR marker. Strains Schu4 and Japan wereincluded as outgroup subspecies for creation of the dendrogram.
western Black Sea region of Turkey so far. This study is the
nomical and travel relations between the two countries may
first to investigate this important issue.
explain the spreading this genotype. Also, immigrant birds
A standardized broth dilution method and susceptibility
or ticks on the birds may transport the causative agent from
breakpoints for F. tularensis were defined for the suscepti-
country to country, and infected mice may enter merchant
bility tests. There is no consensus about diffusion methods,
ships or vehicles and cause the distribution of isolates to other
although diffusion tests have been applied in susceptibility
countries. Another possibility is that the six-locus MLVA is
studies. Tomaso et al. (8) and Ikaheimo et al. (9) harvested
incapable of discriminating these very closely related iso-
the bacteria with turbidity equivalent to that of McFarland
lates. More in-depth analyses including more VNTR mark-
standard 1 and 0.5 into the media of cysteine heart agar supple-
ers and isolates are needed to confirm this unusual genetic
mented with 10% sheep blood agar and medium of cystein
heart agar with 2% hemoglobin, respectively. We testedsusceptibilities in the antibiotic-free medium mentioned for
REFERENCES
culturing. Susceptibilities of the isolates in the present study
¸. (2007): Francisella tularensis and tularemia in Turkey.
and those of Tomaso et al. (8), which were determined by E-
Mikrobiyol. Bul., 41, 621-636 (in Turkish).
test, are similar in that they were susceptible to tetracyclines,
2. Ministry of Health of Turkey: Distribution of Communicable Diseases
aminoglycosides, quinolones, and rifampicin. The Turkish
(Group C) according to Notification System of Cities, Turkey, 2005.
isolates were likely F. tularensis subsp. holarctica biovar
Online at <http://www.saglik.gov.tr/extras/istatistikler/temel2005/tablo-
II because of erythromycin resistance determined by disk
64devam3.htm>. Accessed 19 September 2007 (in Turkish).
3. Gediko˘glu, S., Göral, G. and Helvacı, S. (1990): Epidemiologic aspects
of tularemia in Bursa. ˙Infeksiyon Dergisi, 4, 9-15 (in Turkish).
Kantardjiev et al. (5) described a tularemia outbreak that
¸., Kolayli, F., et al. (2005): Outbreak of
affected almost 300 people in Bulgaria. Ten isolates were iso-
tularaemia in Golcuk, Turkey in 2005: Report of 5 cases and an over-
lated from different sources that appeared to be closely related
view of the literature from Turkey. Scand. J. Infect. Dis., 37, 712-716.
5. Kantardjiev, T., Ivanov, I., Velinov, T., et al. (2006): Tularemia out-
according to the data obtained by amplified fragment length
break, Bulgaria, 1997 - 2005. Emerg. Infect. Dis., 12, 678-680.
polymorphism typing. In the present study, we performed high
6. Byström, M., Böcher, S., Magnusson, A., et al. (2005): Tularemia in
MLVA to compare the Bulgarian and Turkish isolates from
Denmark: identification of a Francisella tularensis subsp. holarctica
the two outbreaks and to shed some light on the genotypic
strain by real-time PCR and high-resolution typing by multiple-locus
structure of F. tularensis populations in the Balkans and
variable-number tandem repeat analysis. J. Clin. Microbiol., 43, 5355-5358.
Anatolia. The two Turkish isolates were identical to one of
7. Johansson, A., Farlow, J., Larsson, P., et al. (2004): Worldwide genetic
the Bulgarian outbreak clusters (see Fig. 1), which is inter-
relationships among Francisella tularensis isolates determined by
esting given that the two outbreaks occurred in regions over
multiple-locus variable-number tandem repeat analysis. J. Bacteriol.,
1,000 km from one another. We think that a common Balkan
8. Tomaso, H., Al, D.S., Hofer, E., et al. (2005): Antimicrobial suscepti-
genotype could exist in Eurasia (Thrace and Anatolia). From
bilities of Austrian Francisella tularensis holarctica biovar II strains.
a historical perspective, the Bulgarian and Turkish people had
Int. J. Antimicrob. Agents, 26, 279-284.
been living in the same geographic location for several
9. Ikaheimo, I., Syrjala, H., Karhukorpi, J., et al. (2000): In vitro anti-
centuries, and relationships between Bulgarian and Turkish
biotic susceptibility of Francisella tularensis isolated from humans and
people continue in the present day. Therefore, the close eco-
animals. J. Antimicrob. Chemother., 46, 287-290.
US Food & Drug Administration FDA Talk Paper FDA Talk Papers are prepared by the Press Office to guide FDA personnel in responding with consistency and accuracy to questions from the public on subjects of current interest. Talk Papers are subject to change as more information becomes available. Broadcast Media: 301-827-3434Consumer Inquiries: 888-INFO-FDA BAYER VOLUNTARILY WITHDRAWS BAYC
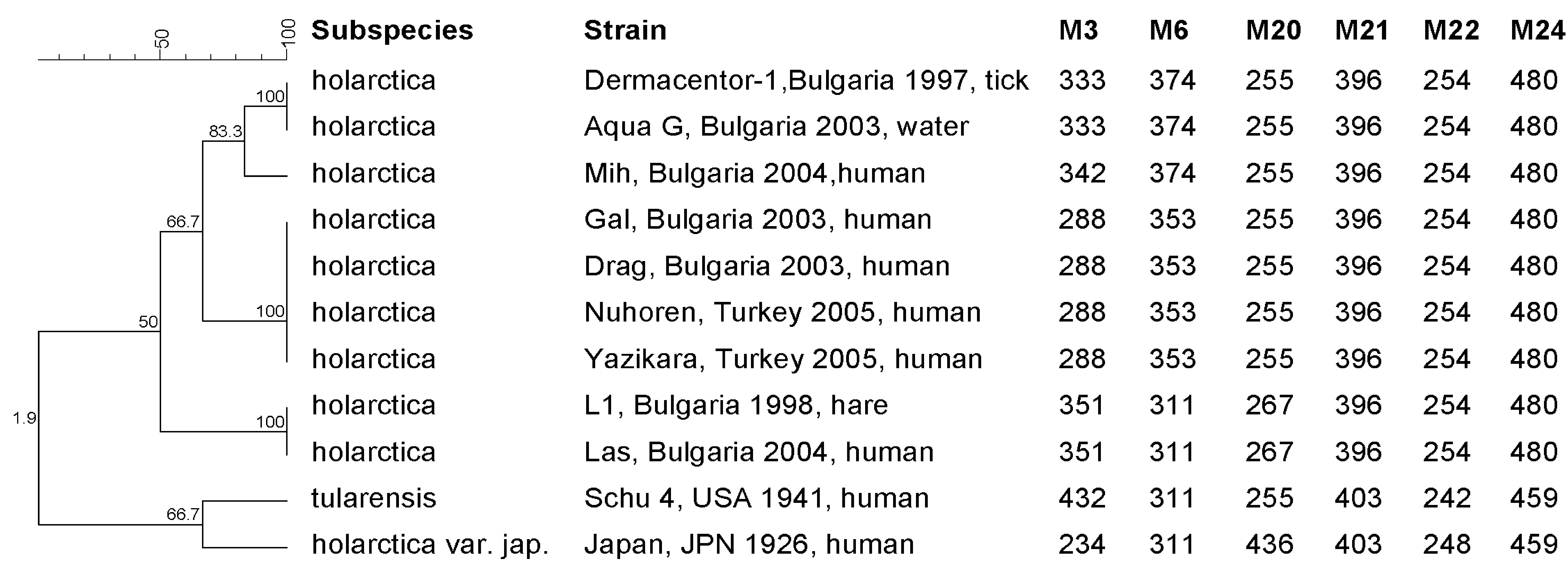 Fig. 1. MLVA cluster analysis of Bulgarian and Turkish Francisella tularensis strains comprising six VNTR loci (M3 to
M24). The corresponding fragment sizes (in base pairs) are given below each VNTR marker. Strains Schu4 and Japan wereincluded as outgroup subspecies for creation of the dendrogram.
Fig. 1. MLVA cluster analysis of Bulgarian and Turkish Francisella tularensis strains comprising six VNTR loci (M3 to
M24). The corresponding fragment sizes (in base pairs) are given below each VNTR marker. Strains Schu4 and Japan wereincluded as outgroup subspecies for creation of the dendrogram.