Tadalafil entfaltet seine Wirkung über eine selektive Hemmung der PDE5, wodurch die Konzentration von cGMP im glatten Muskelgewebe stabil bleibt. Diese biochemische Modulation resultiert in einer langanhaltenden Relaxation der Gefäßwände. Der Wirkstoff wird nach oraler Einnahme effizient resorbiert, mit einer Bioverfügbarkeit von rund 80 %. Seine Halbwertszeit von bis zu 36 Stunden ist innerhalb dieser Substanzklasse außergewöhnlich. Abgebaut wird er in der Leber, hauptsächlich durch CYP3A4, mit anschließender biliärer Exkretion. Typische unerwünschte Wirkungen entstehen durch eine verstärkte Vasodilatation, etwa Kopfschmerzen oder Flush. Pharmakologisch wird cialis generika vor allem durch die verlängerte Wirkungsdauer charakterisiert.
Randomized double-blind controlled study with sublingual carbamylated allergoid immunotherapy in mild rhinitis due to mites
Randomized double-blind controlled study with sublingualcarbamylated allergoid immunotherapy in mild rhinitis due tomites
Background: The clinical efficacy of sublingual immunotherapy (SLIT) in mite
allergy and in mild disease is still a matter of debate, thus we performed a long-
Methods: The study was randomized, double-blind and placebo-controlled.
After a 1-year assessment, 68 patients with mild rhinitis with/without asthma
due to mites were randomized to drugs + placebo or drugs + SLIT for 2 years.
1Allergy and Respiratory Diseases, Department of
Sublingual immunotherapy was given as soluble tablets of monomeric car-
Internal Medicine, University of Genoa, Genoa;
bamylated allergoid. Clinical scores for asthma and rhinitis (0, absent to 3,
2Allergy Unit, Bordighera Hospital, Imperia; 3Allergy
severe) and drug consumption were assessed by diary card in the period
Service, Department of Internal Medicine, S. Orsola
November–February. Quality of life was assessed before and after each obser-
Hospital FBF, Brescia; 4Psychology Unit, Scientific
vation period and pharmaco-economy data were evaluated as well.
Institute of Montescano, S. Maugeri FoundationIRCCS, Montescano (PV), Italy; 5Lofarma S.p.A.,
Results: Fifty-six patients completed the study. The rate of dropouts was similar
in the two groups. No relevant side effect was reported. There was a significantreduction of total clinical scores (P < 0.05) in the active group vs placebo at thefirst year, but not at the second whereas nasal obstruction significantly improvedin both years (P < 0.05). The reduction of drug intake score was significant only
Key words: asthma; carbamylated allergoid; mite
at the first year. No change was observed concerning most of the Short Form-36
allergy; rhinitis; sublingual immunotherapy.
items, because at baseline all patients displayed a normal profile. A significant
change in SLIT group was seen for the item Ôchange in health statusÕ. The need
for extra visits was significantly lower in the active group (25% vs 43%).
Conclusions: Sublingual immunotherapy was clinically effective and safe in mite-
Allergen-specific immunotherapy (IT) is a cornerstone in
that SLIT was a viable alternative to the injection route
the management of respiratory allergy (1), and its clinical
(1). These conclusions were subsequently confirmed in the
value is nowadays well recognized. In general, the clinical
recent ARIA (allergic rhintis and its impact on asthma)
efficacy (reduction of symptoms and need for medica-
guidelines that extended the indication of SLIT to
tions) of IT seems to be greater in pollen than in mite-
children also (8). Also in the case of SLIT, the effects in
induced allergy (1–4). This is probably due to the fact that
mite respiratory allergy were quantitatively less relevant
in the case of dust mite allergy the continuous, although
than in pollen allergy, and statistically significant results
variable, exposure to an allergen sustains a chronic
were often obtained only with long-term treatments (9–
inflammation where the role of immunoglobulin E (IgE)
11). Moreover, in children, SLIT proved effective only in
and mast cells is less relevant than in pollinosis.
those subjects with more severe rhinitis symptoms (12).
Starting from the earliest attempts, IT has been
Therefore, there are still some concerns about the
administered subcutaneously but due to safety aspects
indications and efficacy of SLIT in mild disease.
(5, 6) in the last 20 years new routes of administration
To date, it is recognized that the simple measurement
have been investigated (7) and developed. Among these,
of objective parameters or symptomatic changes does not
the sublingual route (sublingual immunotherapy, SLIT)
provide a full evaluation of the effects of a given
appeared to be the most promising alternative to the
treatment, but the patientsÕ perception also plays a
traditional IT. In 1998, the World Health Organization
relevant role. This is the reason why the assessment of
based on an extensive review of the literature, concluded
quality of life (QoL) is assuming a more and more
important role in clinical trials, especially in allergy (13,
in the Mediterranean area); (vii) any specific IT course in the last
14). In association with the patientsÕ perception of the
5 years and (viii) major psychiatric disorders. All patients signed an
impact of disease on his/her life, there is an another
informed consent at the time of enrollment. A physician was alwaysavailable at each centre for phone contact. All patients were
parameter that can provide further information about the
instructed, as routinely done, to carry on allergen avoidance: use of
subject’s well-being: the so-called ÔsatisfactionÕ that is the
impermeable mattress and pillow covers, removal of moquettes,
cognitive product of the comparison between expecta-
carpets and curtains, hot water washing of bedding once weekly.
tions and reality (15, 16). In the case of IT in general, andSLIT in particular, there are few data concerning the QoLaspects (11). Aim of the present study was to evaluate the
Immunotherapy and concomitant medications
clinical efficacy and the safety of SLIT over a 2-year
Sublingual immunotherapy was a monomeric carbamylated aller-
period in patients suffering from mild rhinitis due to dust
goid (LaisÒ) kindly provided by Lofarma S.p.A. (Milan, Italy)
mites. The effects on QoL were assessed as well.
biologically standardized (9, 19) in allergenic units (AU), and pre-pared as soluble tablets. The tablets had to be taken in the morningon an empty stomach, and kept under the tongue for 1–2 min untildissolution before swallowing. During the build-up phase of about
1 month, tablets with increasing dosages (25, 100, 300 and1000 AU) were used in order to gradually achieve the maximum
dose of 1000 AU. Subsequently, that maintenance dose of 1000 AUwas administered two times a week for 2 years continuously. Con-
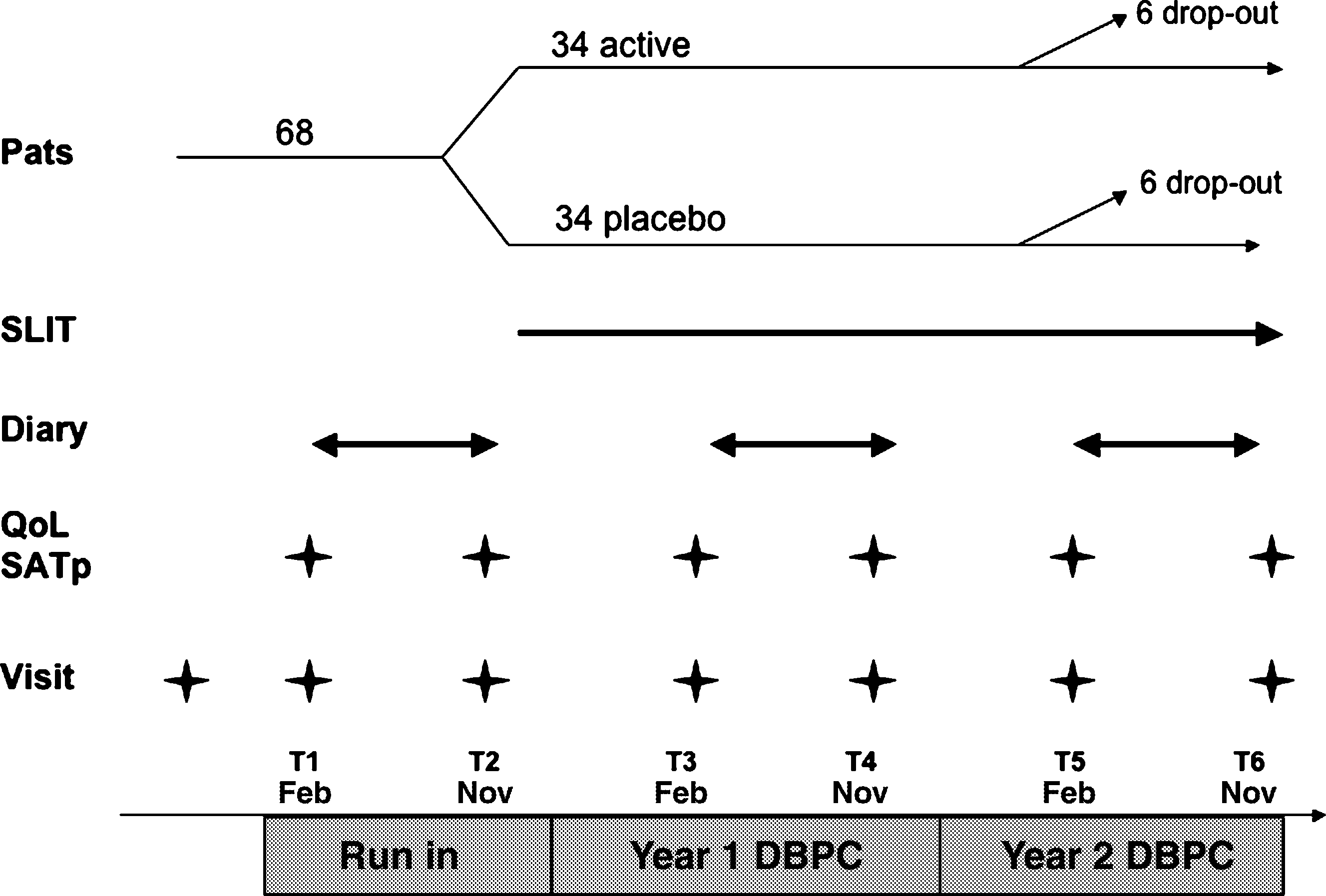
This was a multicentre, randomized, placebo-controlled, two par-
cerning the content of major allergen, it is not reported on the
allel-arm trial of SLIT to mites. Outpatients suffering from mild
product label because the chemical modification of the allergen does
allergic rhinoconjunctivitis with/without mild intermittent asthma
not allow its titration in micrograms. Placebo tablets contained the
were enrolled. All patients underwent a 1-year run-in observation in
same excipients without the allergoid and were undistinguishable
order to establish their baseline clinical conditions. After the run-in,
in aspect, flavour and dissolution time from the active treatment.
patients were randomized to receive, in addition to drug treatment,
Patients were randomly allocated to SLIT or placebo according to a
either SLIT in tablets or matched placebo. Clinical scores (symp-
toms and drug intake) were recorded each year by diary card from
During the study, all patients were allowed to use rescue medi-
November through February. Quality of life and satisfaction were
cations for symptom control: cetirizine tablets (10 mg; once daily),
assessed at regular intervals during the study. The study plan is
inhaled albuterol (100 lg; 2–4 puff on demand), intranasal flutica-
shown in Fig. 1. The trial was approved by the ethical committees
sone (50 lg; 1 spray per nostril once daily on medical prescription).
In the case of severe rhinitis unresponsive to the standard treatment,a short course of systemic steroid was given (prednisone 50 mg daily
Adult patients (18–50 years) of both sexes were enrolled. They had
to suffer from mild persistent rhinitis according to ARIA guidelineswith/without mild intermittent asthma according to Global Initiative
Patients were required to record daily on a specific form the pres-
on Asthma (GINA) guidelines (17) since at least 2 years. They had to
ence and severity of symptoms and the amount of medications used.
have a skin positivity to house dust mite (wheal diameter > 5 mm)
The diary had to be filled from November to February, when the
(18) and a CAP-radioallergosorbent class II or greater. Exclusion
exposure to indoor mites is expected to be greater, for 3 years
criteria were: (i) systemic immunological disorders; (ii) malignancies;
(1 year run-in and 2 years of double-blind study). The following
(iii) diabetes; (iv) chronic heart failure or chronic obstructive pul-
symptoms were considered: nasal itching, obstruction, rhinorrhea,
monary disease; (v) pregnancy or lactation; (vi) skin test positivity to
sneezing, ocular itching, cough and shortness of breath. A score
cat/dog dander or Parietaria (this latter allergen is almost perennial
ranging from 0 (absent) to 3 (severe) was attributed daily to each ofthe mentioned symptoms. A mean daily score was calculated foreach 4-month period. The drug intake was scored 1 point for eachactuation of salbutamol, 2 points for each dose of antihistamine,nasal or inhaled steroid, 3 points for each dose of systemic steroid,and a cumulative drug intake score was obtained.
All patients were also required to record on a separate diary any
untoward effect, possibly related to the intake of SLIT. Adverseevents were subdivided into local (oral itching, swelling of tongue)and systemic: asthma, rhinitis, urticaria, abdominal pain/diarrhoeaand anaphylaxis. Finally, patients had to record the number of extravisits (other than the scheduled ones) attended, and the working(school) days missed because of their allergy problems.
At the beginning and the end of each observation period (Novemberand February), patients had to fill two generic questionnaires, oneassessing the health status and the other one assessing the subjective
satisfaction. The QoL was measured by the Short Form (SF)-36Health Survey, a generic, widely used questionnaire, already valid-ated in allergic respiratory disease. It consists of 36 items corres-ponding to eight domains: physical function, role limitation(physical), bodily pain, general health, vitality, social function, rolelimitation (emotional) and mental health. An additional questioninvestigates a general evaluation of perceived changes in healthstatus in the past year. The satisfaction was evaluated by the SAT-P,a nondisease specific tool with 32 questions about several aspects ofdaily life. The patients indicate their subjective satisfaction on a10 cm visual analogue scale, from 0 (extremely dissatisfied) to 10(extremely satisfied). The SATisfaction profile (SAT-P) provides ananalytic score about the 32 items and a score about the five factorsextracted: psychological functioning, physical functioning, work,sleep/eating/leisure and social functioning. The SAT-P has beenpreviously used in patients with allergic diseases (16, 20).
The nonparametric tests for two independent samples are useful for
Figure 2. Mean ± SD daily total symptom score in the active
determining whether or not the values of a particular variable (i.e.
and placebo group at baseline and after 1 and 2 years of
total symptom score) differ between two groups (SLIT vs placebo).
This is especially true when the assumptions of the t-test are notmet. We used the Mann–Whitney and Wilcoxon statistics to test thenull hypothesis that two independent samples came from the samepopulation. Their advantage over the independent samples t-test isthat Mann–Whitney and Wilcoxon do not assume normality andcan be used to test ordinal variables.
Sixty-eight patients were enrolled in the trial. Their meanage was 31.28 ± 8.14 years, with an age range of 18–49,and 41.2% of them were male. Twelve patients, six ineach group, dropped out, mainly during the run-in phase. Two subjects from the placebo group withdrew forconcomitant illness, nine patients (four placebo and fiveactive) retired their informed consent for personal reasonsand one active patient dropped out for major protocoldeviation (unattended visits). Fifty-six patients (mean age32.14 ± 7.97 years, 39.3% male) completed the study.
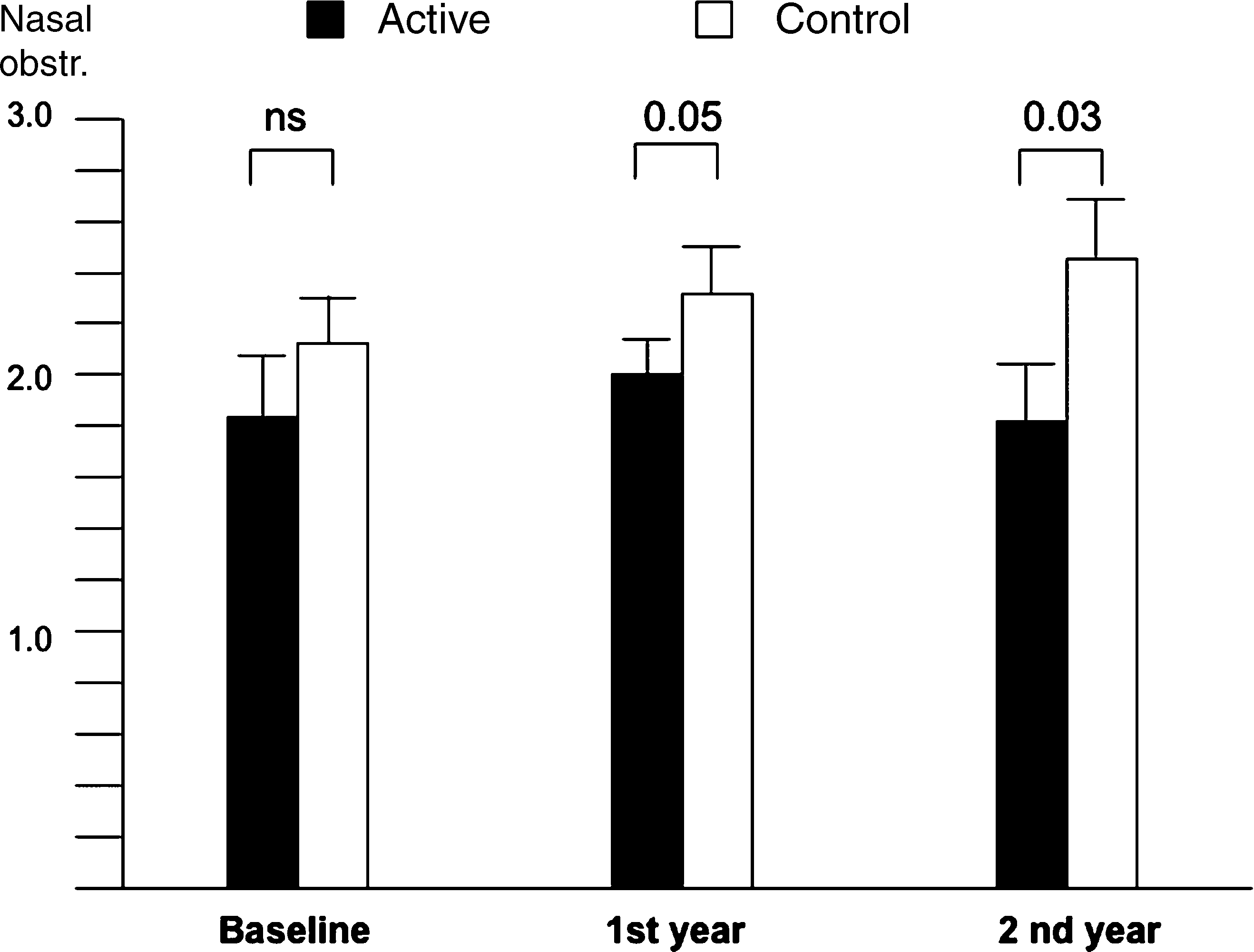
Figure 3. Mean ± SD daily obstruction score in the active andplacebo group at baseline and after 1 and 2 years of treatment.
The patients were homogeneous at baseline for demo-graphy and clinical characteristics (Table 1).
considered acceptable. Fig. 2 shows the mean daily
clinical score (all symptoms) at baseline, after 1 and
Due to the very long duration of the study, a rate of
2 years of treatment. A significant difference between the
<15% of missing data in the clinical diaries was
two groups could be found after 1 year of treatment(P ¼ 0.027), whereas no statistical difference was found
Table 1. Demographics and clinical characteristics by treatment group
at the second year, although a trend towards improve-ment was seen. Concerning the symptom Ônasal obstruc-
tionÕ a significant difference between groups was present
after 1 year (P ¼ 0.05) and 2 years (P ¼ 0.033) of treat-
ment (Fig. 3). No difference during the study could be
found for the other symptoms taken separately. The
global drug intake is shown in Fig. 4, being the difference
significant at the first year of treatment (P ¼ 0.036), but
not at the second, although a trend toward difference was
Quality of life, satisfaction profile and pharmaco-economics
There was no statistical change in all the domains of theSF-36 questionnaire at the six timepoints, and all thescores were quite high. Table 3 shows the values for eachdomain that are not different from those of a referencehealthy population (21–23). There was indeed a differencebetween the active and the placebo group in the only itemÔoverall change in health statusÕ (P ¼ 0.05) after thesecond year of treatment (Fig. 5). No change in the itemsof the SAT-P questionnaire was found, because in thiscase also the scores were always comparable with those ofa healthy reference group ( data not shown).
There was a significant difference between the two
groups as far as the pharmaco-economic aspects areconcerned. No working absence was reported in theactive group. In the placebo group, three patientsreported a total of 22 working days lost attributable to
Figure 4. Mean ± SD of the drug intake in the considered 4-
their allergic disease. This means a cost of 3047€ (138.5€
per day) (24) that is superior to the cost of SLIT for thesame number of patients (about 2700€). Moreover, 12
seen. Nasal steroids were prescribed only occasionally in
patients (43%) in the placebo group and six patients
both groups and a statistical analysis was not therefore
(25%) in the active group needed one or more extra visit
(P ¼ 0.01) due to illness exacerbation.
The occurrence of adverse events was not significantly
different between the two groups. Thirty events (11patients) in the actively treated and 43 events (16 patients)in the placebo group were reported and none was judged
possibly or certainly related to treatment. A list of those
The use and indication of SLIT in mite allergy are less
adverse events occurring at least twice is shown in
defined than in pollinosis. In fact, the results of clinical
Table 2. In the active group, two patients reported
trials are less apparent in term of efficacy and need longer
transient oral itching and one patient mild abdominal
times to become measurable. Some clinical trials have
provided positive results (9–11, 25), whereas in otherstudies the effects were marginal (26) or absent (27, 28).
Table 2. Detail of the adverse events occurring more than one time
This may be due to the fact that with mites the allergenic
exposure is extremely variable during the course of theyear and therefore, prolonged periods of observation are
needed. Furthermore, mite-induced allergy may provoke
less severe symptoms, although long-lasting. It is difficult
to carry out studies with mite allergy in adult patients. In
fact, it is objectively difficult to keep many patients on a
double-blind design, recording symptoms and drug intake
Table 3. Short Form-36 domains score at the six timepoints in the active and placebo group
The last column on the right shows the mean values for a reference healthy population (19).
23), so it was not conceivable to obtain an improvementof normal values. Thus, we can deduce that a mild diseasedoes not significantly affect the QoL of patients or, inother words, patients with mild symptoms cope with theirdisease and do not perceive an impact on daily function-ing. This fact, indirectly confirms the validity of theARIA classification of the severity of rhinitis. In addition,it has been previously shown that generic questionnaires(e.g. the SF-36) may be unable to detect changes in healthstatus (29). On the other hand, a significant change in theitem exploring the variation of the disease’s status wasfound and a statistical projection showed that this changewould have been maintained and would have becomemore and more significant in the next years. Of note,there was also a difference in extra visits and workingabsence in the active group, this indirectly testifying thata general effect on the disease severity has occurred. Itremains to be ascertained whether a continuous SLITtreatment in mild disease can be proposed to all patientsin clinical practice, although the adherence to treatmentwas shown not to represent a problem (30).
Figure 5. Short Form-36 scores Ôchange in health statusÕ meas-
The clinical effect of SLIT also in mild disease should
be considered in the light of the very favourable tolerab-ility profile that would also allow small children to be
continuously for years. We therefore chose to record the
safely treated (31). In this study, the safety aspect was
clinical scores only 4 months a year, from November to
further ensured by the use, as active principle, of a
February, when the exposure to allergens was expected to
monomeric carbamylated allergoid, which has a reduced
be higher. With this method, we could demonstrate that
IgE-binding capacity. The monomeric carbamylated
allergoid SLIT induced a significant improvement of total
allergoid resulted to be very suitable for SLIT treatments
clinical symptoms and drug consumption at the first year,
because on the one hand its low molecular size (19) allows
whereas in the second year no significance was reached.
absorption at the mucosal level and on the other, the
This is consistent with the fact that all patients had a mild
carbamylation improves its bioavailability by increasing
disease, and were allowed to use rescue medications for
the resistance to enzymatic degradation at the gastroin-
their symptoms. On the other hand, the symptom Ônasal
testinal level, as shown by biodistribution studies per-
obstructionÕ that is the most bothering symptom of
formed with the radiolabelled Der p 2 (32). In conclusion,
persistent rhinitis, especially in patients allergic to peren-
SLIT with carbamylated allergoid exerts a measurable
nial allergens like mites, was improved in both the
clinical effect even in mild rhinitis due to mites, and
observation periods. Obstruction in persistent forms is
favourably affects the pharmaco-economic profile of the
largely sustained by inflammation, and the improvement
of obstruction is consistent with the previously demon-strated anti-inflammatory action of the allergoid IT (9). The nonsignificant difference between the two groups at
baseline did not affect the final results as confirmed by atime-trend analysis.
This work was partially supported by ARMIA (AssociazioneRicerca Malattie Immunologiche e Allergiche). We thank biostat-
Concerning QoL, all patients had QoL profiles not
istician Dr Giorgio Reggiardo for his precious help.
different from a control group of healthy subjects (15, 21–
2. Malling HJ. Allergen-specific immuno-
Allergy Clin Immunol 2001;1:43–46.
allergic rhinitis. Cochrane Database Syst
5. Committee on the safety of medicines.
25. Ippoliti F, De Sanctis W, Volterrani A,
Lenti L, Canitano N, Lucarelli S et al.
Allergy Clin Immunol 1993;92:6–15.
therapy in allergic children. Pediatr Al-
Allergy Clin Immunol 2003;111:437–448.
Giardini A, Viola L, Baiardini I et al. A
new instrument in quality of life assess-
(editors). Allergic Rhinits and its Impact
ment: the Satisfaction Profile. Int J Ment
17. GINA. Global Initiative on Asthma.
Riccio A, Pronzato C, Mela GS et al.
tee on skin tests. Skin tests used in type I
mite extracts in children. Pediatr Allergy
junctivitis. Lancet 1998;351:629–632.
28. Guez S, Vatrinet C, Fadel R, AndreÕ C.
double blind placebo controlled study.
characterization. Allergy 1996;51:8–15.
double-blind, placebo-controlled study.
Dignetti P, Guerra L, Specchia C et al.
Quality of life and patient’s satisfaction
health status in allergic rhinitis? Allergy
Dei Risultati. Milan: Guerini, 1997.
adherence to sublingual immunotherapy.
12. Bufe A, Ziegler-Kirbach E, Stoeckmann
Senna GE, Minale P, D’Ulisse S et al.
Minelli M, Pecora S, Canonica GW et al.
double-blind placebo-controlled study.
13. Meltzer EO. Quality of life in adults and
children with allergic rhinitis. J Allergy
goid in allergic volunteers. Int Arch Al-
Ordinaria Dei Partecipanti. Roma:Banca D’Italia, 2003.
.exchange.atla.or Visit the Exchange online Professional Negligence Volume 18, Number 1 February 2003 Law: Negligence claim does not accrue until criminal proceedings are final, page 3 Gynecology: Failure to order mammogram for patient with family history of breast cancer, page 4 FTCA Liability: Failure to diagnose bacterial meningitis, page 5 Nursing Home: Failure
These instructions are designed to inform you about Total Knee Replacement. Initial instructions are to be fol owed before the surgery, during your stay in the hospital and after surgery when you are at home. The success of the Total Knee Replacement surgery requires active participation of the patient. For a long-term successful result, understanding and adherence to these guidelines are imper
 important role in clinical trials, especially in allergy (13,
in the Mediterranean area); (vii) any specific IT course in the last
14). In association with the patientsÕ perception of the
5 years and (viii) major psychiatric disorders. All patients signed an
impact of disease on his/her life, there is an another
informed consent at the time of enrollment. A physician was alwaysavailable at each centre for phone contact. All patients were
parameter that can provide further information about the
instructed, as routinely done, to carry on allergen avoidance: use of
subject’s well-being: the so-called ÔsatisfactionÕ that is the
impermeable mattress and pillow covers, removal of moquettes,
cognitive product of the comparison between expecta-
carpets and curtains, hot water washing of bedding once weekly.
important role in clinical trials, especially in allergy (13,
in the Mediterranean area); (vii) any specific IT course in the last
14). In association with the patientsÕ perception of the
5 years and (viii) major psychiatric disorders. All patients signed an
impact of disease on his/her life, there is an another
informed consent at the time of enrollment. A physician was alwaysavailable at each centre for phone contact. All patients were
parameter that can provide further information about the
instructed, as routinely done, to carry on allergen avoidance: use of
subject’s well-being: the so-called ÔsatisfactionÕ that is the
impermeable mattress and pillow covers, removal of moquettes,
cognitive product of the comparison between expecta-
carpets and curtains, hot water washing of bedding once weekly.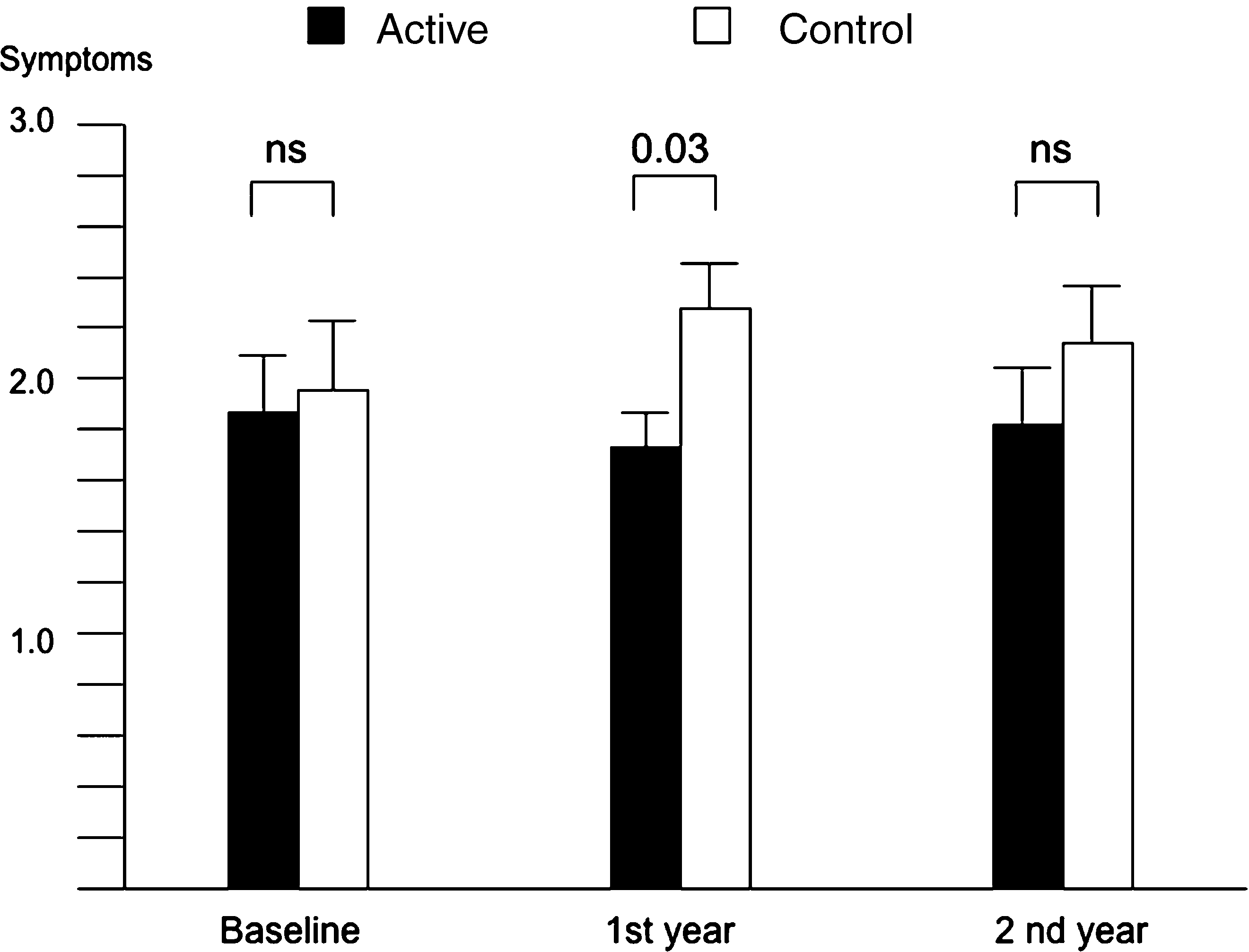
 satisfaction. The QoL was measured by the Short Form (SF)-36Health Survey, a generic, widely used questionnaire, already valid-ated in allergic respiratory disease. It consists of 36 items corres-ponding to eight domains: physical function, role limitation(physical), bodily pain, general health, vitality, social function, rolelimitation (emotional) and mental health. An additional questioninvestigates a general evaluation of perceived changes in healthstatus in the past year. The satisfaction was evaluated by the SAT-P,a nondisease specific tool with 32 questions about several aspects ofdaily life. The patients indicate their subjective satisfaction on a10 cm visual analogue scale, from 0 (extremely dissatisfied) to 10(extremely satisfied). The SATisfaction profile (SAT-P) provides ananalytic score about the 32 items and a score about the five factorsextracted: psychological functioning, physical functioning, work,sleep/eating/leisure and social functioning. The SAT-P has beenpreviously used in patients with allergic diseases (16, 20).
satisfaction. The QoL was measured by the Short Form (SF)-36Health Survey, a generic, widely used questionnaire, already valid-ated in allergic respiratory disease. It consists of 36 items corres-ponding to eight domains: physical function, role limitation(physical), bodily pain, general health, vitality, social function, rolelimitation (emotional) and mental health. An additional questioninvestigates a general evaluation of perceived changes in healthstatus in the past year. The satisfaction was evaluated by the SAT-P,a nondisease specific tool with 32 questions about several aspects ofdaily life. The patients indicate their subjective satisfaction on a10 cm visual analogue scale, from 0 (extremely dissatisfied) to 10(extremely satisfied). The SATisfaction profile (SAT-P) provides ananalytic score about the 32 items and a score about the five factorsextracted: psychological functioning, physical functioning, work,sleep/eating/leisure and social functioning. The SAT-P has beenpreviously used in patients with allergic diseases (16, 20).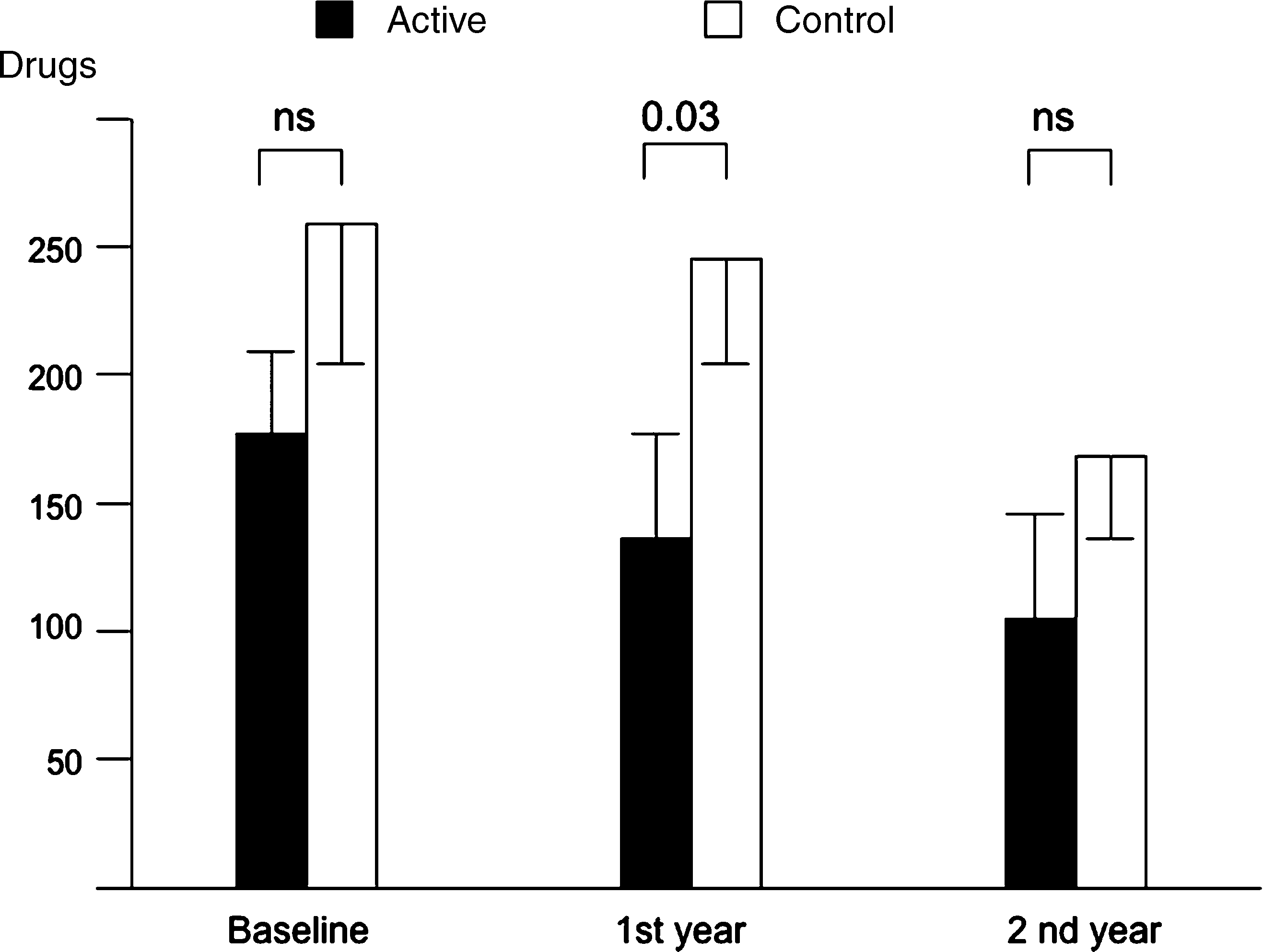 Quality of life, satisfaction profile and pharmaco-economics
There was no statistical change in all the domains of theSF-36 questionnaire at the six timepoints, and all thescores were quite high. Table 3 shows the values for eachdomain that are not different from those of a referencehealthy population (21–23). There was indeed a differencebetween the active and the placebo group in the only itemÔoverall change in health statusÕ (P ¼ 0.05) after thesecond year of treatment (Fig. 5). No change in the itemsof the SAT-P questionnaire was found, because in thiscase also the scores were always comparable with those ofa healthy reference group ( data not shown).
Quality of life, satisfaction profile and pharmaco-economics
There was no statistical change in all the domains of theSF-36 questionnaire at the six timepoints, and all thescores were quite high. Table 3 shows the values for eachdomain that are not different from those of a referencehealthy population (21–23). There was indeed a differencebetween the active and the placebo group in the only itemÔoverall change in health statusÕ (P ¼ 0.05) after thesecond year of treatment (Fig. 5). No change in the itemsof the SAT-P questionnaire was found, because in thiscase also the scores were always comparable with those ofa healthy reference group ( data not shown).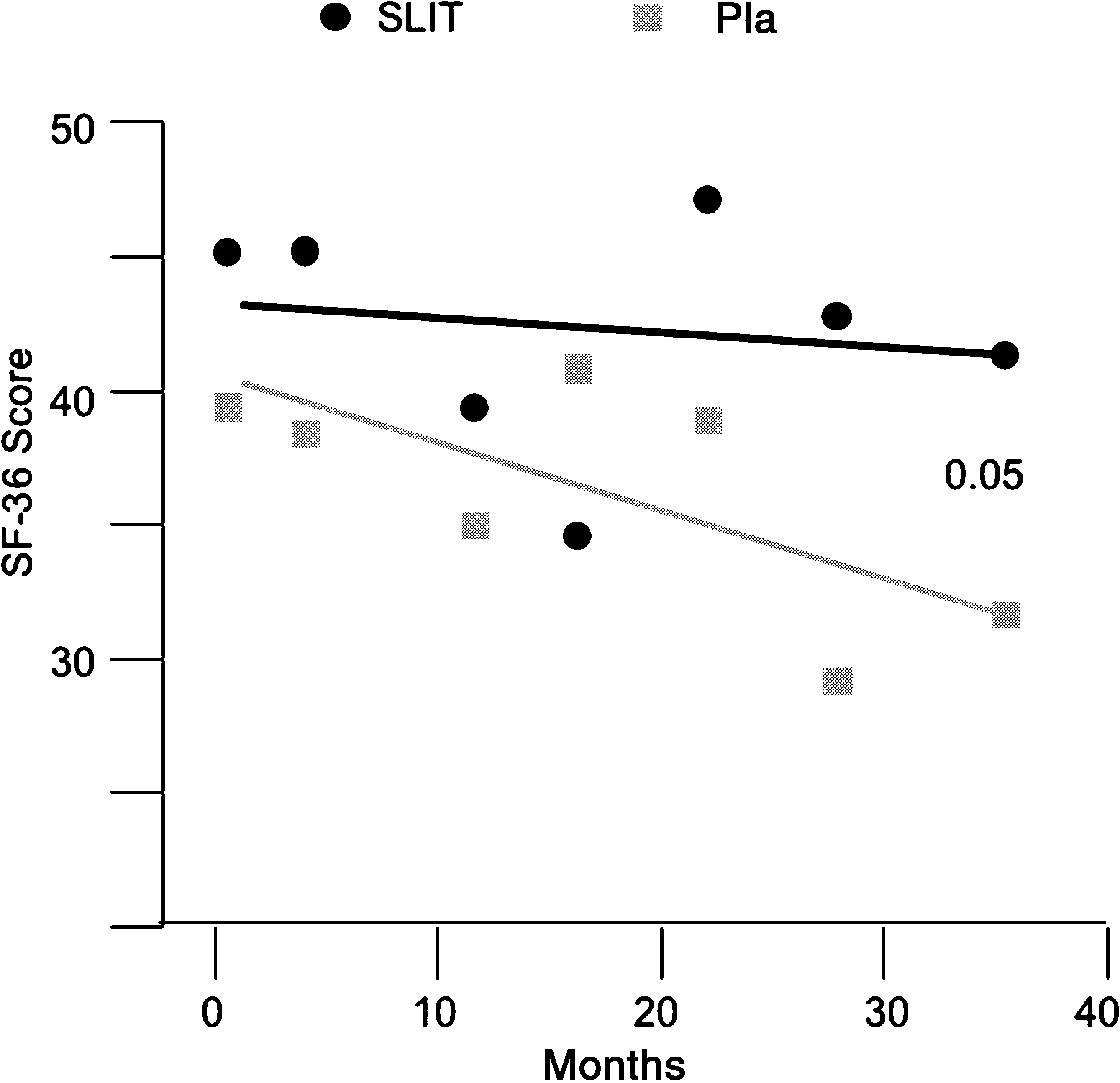 23), so it was not conceivable to obtain an improvementof normal values. Thus, we can deduce that a mild diseasedoes not significantly affect the QoL of patients or, inother words, patients with mild symptoms cope with theirdisease and do not perceive an impact on daily function-ing. This fact, indirectly confirms the validity of theARIA classification of the severity of rhinitis. In addition,it has been previously shown that generic questionnaires(e.g. the SF-36) may be unable to detect changes in healthstatus (29). On the other hand, a significant change in theitem exploring the variation of the disease’s status wasfound and a statistical projection showed that this changewould have been maintained and would have becomemore and more significant in the next years. Of note,there was also a difference in extra visits and workingabsence in the active group, this indirectly testifying thata general effect on the disease severity has occurred. Itremains to be ascertained whether a continuous SLITtreatment in mild disease can be proposed to all patientsin clinical practice, although the adherence to treatmentwas shown not to represent a problem (30).
23), so it was not conceivable to obtain an improvementof normal values. Thus, we can deduce that a mild diseasedoes not significantly affect the QoL of patients or, inother words, patients with mild symptoms cope with theirdisease and do not perceive an impact on daily function-ing. This fact, indirectly confirms the validity of theARIA classification of the severity of rhinitis. In addition,it has been previously shown that generic questionnaires(e.g. the SF-36) may be unable to detect changes in healthstatus (29). On the other hand, a significant change in theitem exploring the variation of the disease’s status wasfound and a statistical projection showed that this changewould have been maintained and would have becomemore and more significant in the next years. Of note,there was also a difference in extra visits and workingabsence in the active group, this indirectly testifying thata general effect on the disease severity has occurred. Itremains to be ascertained whether a continuous SLITtreatment in mild disease can be proposed to all patientsin clinical practice, although the adherence to treatmentwas shown not to represent a problem (30).