Tadalafil entfaltet seine Wirkung über eine selektive Hemmung der PDE5, wodurch die Konzentration von cGMP im glatten Muskelgewebe stabil bleibt. Diese biochemische Modulation resultiert in einer langanhaltenden Relaxation der Gefäßwände. Der Wirkstoff wird nach oraler Einnahme effizient resorbiert, mit einer Bioverfügbarkeit von rund 80 %. Seine Halbwertszeit von bis zu 36 Stunden ist innerhalb dieser Substanzklasse außergewöhnlich. Abgebaut wird er in der Leber, hauptsächlich durch CYP3A4, mit anschließender biliärer Exkretion. Typische unerwünschte Wirkungen entstehen durch eine verstärkte Vasodilatation, etwa Kopfschmerzen oder Flush. Pharmakologisch wird cialis generika vor allem durch die verlängerte Wirkungsdauer charakterisiert.
Lj180003256p
H i g h S u r v i v a l R a t e i n I n f a n t A c u t e L e u k e m i a T r e a t e d W i t h E a r l y H i g h - D o s e C h e m o t h e r a p y a n d S t e m - C e l l S u p p o r t
By Fernando Marco, Encarna Bureo, Juan J. Ortega, Isabel Badell, Amparo Verdaguer, Ana Martı´nez, Arturo Mun˜oz,
Luis Madero, Teresa Olive´, Josep Cubells, Victoria Castel, Ana Sastre, M. Soledad Maldonado,
and Miguel A. Dı´az from the Grupo Espan˜ol de Trasplante de Me´dula Ósea en Nin˜os
Purpose: Infants with acute leukemia have a poor are 64% (SE ؍ 9%) and 63% (SE ؍ 10%), respectively. prognosis when treated with conventional chemother- Autologous and allogeneic SCT offered similar outcome. apy. It is still unknown if stem-cell transplantation (SCT) There was not any transplant-related mortality, and all can improve the outcome of these patients. In the deaths were caused by relapse in the first 6 months present study, we review our experience with SCT in after SCT. In multivariate analysis, the single factor infant acute leukemia to clarify this issue. associated with better DFS was an interval between Patients and Methods: We report the results of 26 CR1 and SCT of less than 4 months (P < .025). infants who were submitted to a SCT for acute leukemia. Conclusion: SCT is a valid option in the treatment of There were 15 cases of acute myeloid leukemia and 10 infant acute leukemia, and it may overcome the high cases of acute lymphoid leukemia. One patient had a risk of relapse with conventional chemotherapy show- bilineal leukemia. Twenty-two patients were in their first ing very reduced toxicity. This study suggests that SCT complete response (CR1), three were in their second CR, should be performed in CR1 in the early phase of the and one was in relapse. Eight patients were submitted to disease. allogeneic SCT, and 18 underwent autologous SCT. J Clin Oncol 18:3256-3261. 2000 by American Results: With a median follow-up of 67 months, the Society of Clinical Oncology. 5-year overall survival and disease-free survival (DFS)
LEUKEMIASTHATdevelopwithinthefirstyearoflife with conventional chemotherapy regimens, but they show a
have distinctive biologic and clinical features. Infant
high relapse rate, with long-term disease-free survival
acute lymphoblastic leukemia (ALL) is characterized by
(DFS) ranging from 25% to 43% in large cooperative
hyperleukocytosis, hepatosplenomegaly, CNS involvement
group studies.8-12 Despite some recent reports showing
at diagnosis, and CD19ϩ, CD10Ϫ immunophenotype with
an increased DFS for infants with ALL treated with more
myeloid-associated antigen expression.1-3 Acute myeloid
intensive chemotherapy regimens,13,14 outcome for these
leukemia (AML) shows a higher incidence of myelomono-
patients is far from being optimal. The prognosis of
cytic or monocytic phenotypes (M4 or M5) and is fre-
infant AML treated with chemotherapy is not better, with
quently associated with hyperleukocytosis and extramedul-
reported DFS of 31% to 42%.15,16 Thus, autologous or
lary disease.1,4,5 Rearrangements of the MLL gene in
allogeneic bone marrow transplantations (BMT) havebeen tried by some groups to reduce the risk of relapse
chromosome 11q23, including cases with apparently normal
with some encouraging results, although published series
karyotype, have been found in 70% to 80% of infant ALL
and are associated with a poor outcome.1,6-8 In infant AML,
The present study was undertaken to investigate whether
this finding is present in nearly 60% of cases and correlates
an intensive multiagent chemotherapy with stem-cell sup-
with M4 and M5 phenotypes.4 Most infants with ALL
port could improve the DFS of infants with acute leukemia.
achieve complete response (CR) when they are first treated
We retrospectively analyzed the clinical features, treatmentoutcome, and prognostic variables of 26 patients with infantacute leukemia who underwent stem-cell transplantation
From the Hospital Universitario Marque´s de Valdecilla, Santander;
(SCT) in hospitals associated with the Grupo Espan˜ol de
Hospital Materno-Infantil Vall D’Hebro´n; Hospital de la Santa Creu i
Trasplante de Me´dula Osea en Nin˜os. Sant Pau, Barcelona; Hospital Universitario La Fe, Valencia; HospitalLa Paz; Hospital Ramo´n y Cajal; and Hospital del Nin˜o Jesu´s, Madrid,Submitted September 2, 1999; accepted May 5, 2000.Address reprint requests to Fernando Marco, MD, Servicio deHematologı´a, Hospital Universitario Marque´s de Valdecilla, Avenida
From January 1990 to December 1998, 26 SCT were performed in
de Valdecilla 1, 39008 Santander, Spain; email fernandomarco@
patients diagnosed with acute leukemia in the first year of life in seven
Spanish hospitals. Fifteen of these patients had AML, 10 had ALL, and
2000 by American Society of Clinical Oncology.
one had bilineal leukemia. Their pretransplant clinical characteristics
Journal of Clinical Oncology, Vol 18, No 18 (September 15), 2000: pp 3256-3261
Transplantation Diagnosis Characteristics
Median age at diagnosis was 7 months (range, 1 to 12 months).
There were 15 males and 11 females. Three patients had CNSinvolvement at diagnosis, and 20 had hepatosplenomegaly. The median
leukocyte count was 28 ϫ 109/L (range, 1.3 to 900 ϫ 109/L). Immunophenotype was CD19ϩ, CD10Ϫ in 50% of ALL patients.
All patients were engrafted with a median time to an
Cytogenetic studies were available in 14 patients. Four patients had a
absolute neutrophil count of 0.5 ϫ 109/L of 22 days (range,
normal karyotype, six showed anomalies of the 11q23 region, and four
10 to 70 days). A platelet count of 20 ϫ 109/L was achieved
in a median of 31.5 days (range, 16 to 120 days). One
patient, who had received an autologous transplant purgedwith mafosfamide, achieved engraftment only after a second
Most ALL patients had been previously treated with multiagent
infusion of autologous cells on day ϩ40.
chemotherapy protocols that included doxorubicin, cyclophosphamide,vincristine, prednisone, L-asparaginase, intrathecal therapy, and high-
dose methotrexate and cytarabine.21-23 AML patients had been mostlytreated with protocols including at least two cycles of an anthracycline,
Eighteen of 26 patients are alive, with a median survival
cytarabine, and etoposide. The decision to perform SCT was made at
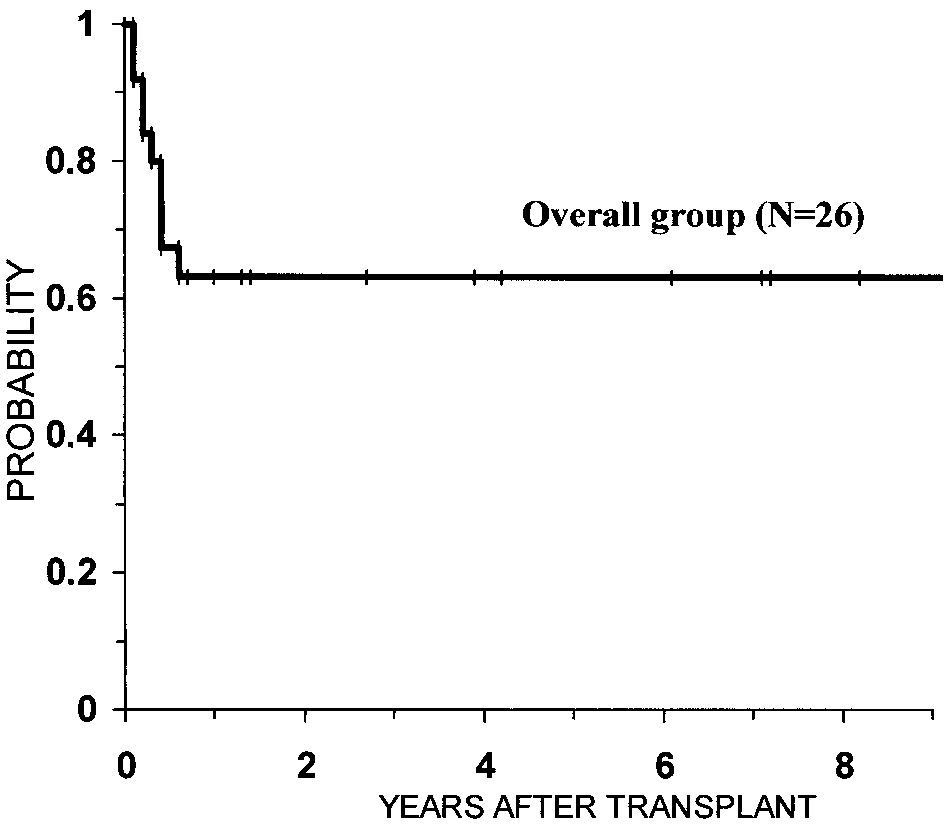
of 67 months. Five-year overall survival and DFS are 64%
the discretion of the responsible physician.
(SE ϭ 9%) and 63% (SE ϭ 10%) (Fig 1), respectively. In
patients transplanted in CR1, DFS is 71% (SE ϭ 10%),whereas only one of four patients transplanted in more
Patient characteristics at the time of BMT are listed in Table 1.
Median time from first CR (CR1) to BMT was 3.5 months (range, 1 to
advanced status survives. Patients with ALL had a 5-year
25 months). Disease status at transplant was CR1 in 22 cases, second
DFS of 56%, and AML patients had a DFS of 73% (P ϭ not
CR (CR2) in three patients, and more advanced disease in one patient.
significant) (Fig 2). Five out of eight recipients of allogeneic
Eight patients received an allogeneic transplant. Donors were six
transplant and 12 of 18 recipients of autologous transplants
HLA-identical siblings, one partially mismatched parent, and one
matched unrelated donor. Eighteen patients who had no suitable donorwere submitted to autologous transplant. The source of progenitors was
In logistic regression using univariate analysis, signifi-
bone marrow in 22 patients, peripheral-blood stem cells in three
cant factors associated with greater DFS were leukocyte
patients, and umbilical cord blood cells in one patient. Election of the
count less than 20 ϫ 109/L at diagnosis (P Ͻ .04) and an
conditioning regimen was made at the discretion of the responsible
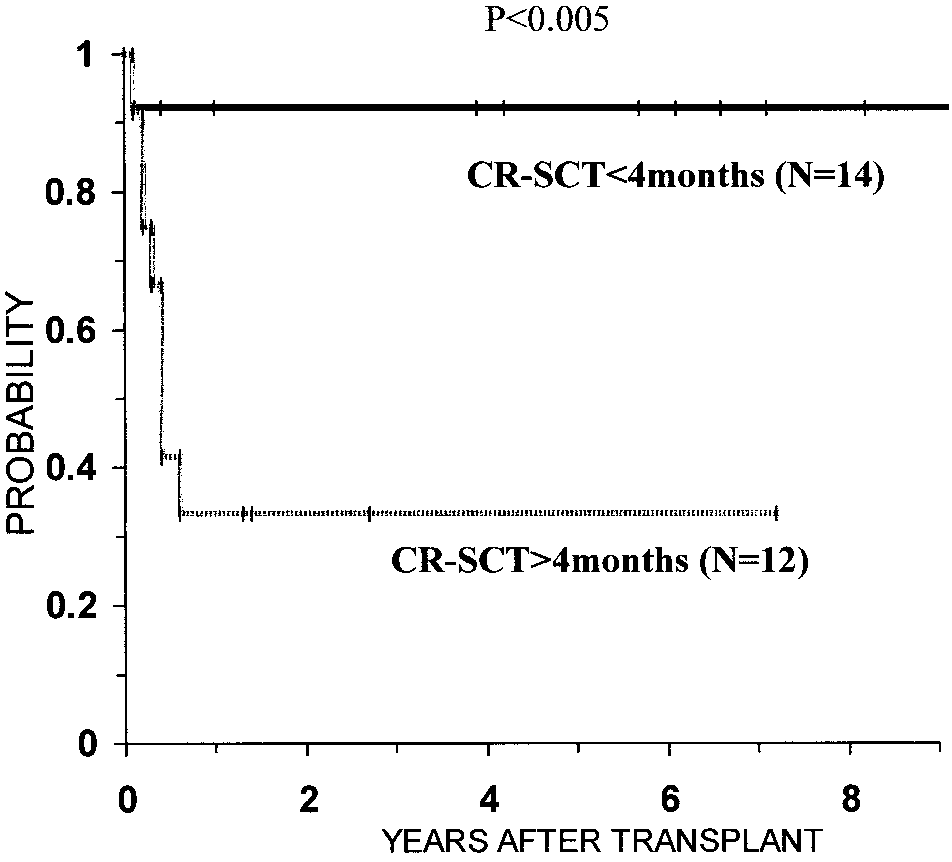
interval between CR1 and SCT of less than 4 months (P Ͻ
physician. Twenty patients received conditioning regimens that in-
.005) (Fig 3). Factors that showed no significant association
cluded busulfan, cyclophosphamide, and, in some patients, etoposide. Only one patient was treated with total-body irradiation, cytarabine,
with DFS included age at diagnosis less than 6 months,
and cyclophosphamide, whereas five patients received other chemo-
therapy regimens. Phenytoin, phenobarbital, or clonazepam were ad-
CD10Ϫ immunophenotype, 11q23 abnormalities in karyo-
ministered to patients who received busulfan for prophylaxis ofseizures. Busulfan levels were not targeted in any patient. All alloge-neic transplant recipients received unmanipulated stem cells. Autolo-gous bone marrow was purged ex-vivo with mafosfamide in sixpatients and with monoclonal antibodies in two. Measures to preventinfection varied according to the standard of practice at the time ofSCT. Eight patients received growth factors after transplantation. Graft-versus-host-disease (GVHD) prophylaxis consisted of cyclospor-ine or short-term methotrexate and cyclosporine. Assessment andgrading of acute and chronic GVHD were performed according tostandard criteria.24 Late adverse effects of SCT, including developmen-tal delay, learning disabilities, and endocrinopathies, were evaluated inall long-term survivors.
Overall survival and DFS were estimated using the Kaplan-Meier
method, with differences between groups being analyzed by thetwo-tailed log-rank test. DFS was calculated from the date at SCT torelapse, death, or last contact. Data from second transplants were notincluded in this study, and recipients were censored for overall survivalat time of second transplant. Cox multivariate analysis was performedto estimate the independent effect of various factors in overall survivaland DFS. Only factors at 5% level from the univariate analysis wereassessed in the multivariate analysis. All analyses were performed with
Fig 1. Kaplan-Meier estimated DFS for overall group of 26 infants
the NCSS statistical package (NCSS, Kaysville, UT). transplanted for acute leukemia.
type, allogeneic SCT, and conditioning regimen. In multi-variate analysis, an interval between CR and SCT of lessthan 4 months was the only significant factor associatedwith greater DFS (P Ͻ .025). In patients transplanted duringthe first 4 months after CR1, DFS is 92% (SE ϭ 8%).
No patient died of transplant-related complications. All
patients developed fever, neutropenia, and low-grade mu-cositis. One patient presented with reversible veno-occlu-sive disease. Grade III/IV acute GVHD was not seen in anyallogeneic recipient, and none of the six patients whosurvived more than 100 days after an allogeneic SCT hadextensive chronic GVHD. Neuropsychologic developmentwas slightly delayed in one patient only after the patient wassubmitted to a second SCT. No other late effects, such asgrowth retardation, cataracts, endocrinopathies, cardiacfunction impairment, or secondary neoplasias, were de-
Fig 3. Kaplan-Meier estimated DFS for patients submitted to SCT within
tected. Long-term survivors are doing intellectually well,
the first 4 months after CR compared with patients transplanted after the first
and most are eventually attending school. 4 months after CR. Statistical significance was determined by the log-rank test.
The only cause of death was leukemic recurrence. Nine
finally died from relapse. No other patients were submitted
patients relapsed, with a median time of 104 days from SCT
to relapse. All relapses were hematologic and occurred inthe first 6 months after SCT. A new remission was obtained
in one relapsed patient who received chemotherapy and a
Several cooperative group studies have stated the role of
second SCT from a different sibling donor. This patient
SCT in the treatment of children with AML25,26 or high-riskALL.27,28 Although infants with ALL or AML are consid-ered to have a poorer outcome when compared with olderchildren, a few small noncomparative series of BMT ininfant acute leukemia have been reported.17-20 Thus, theindication of allogeneic or autologous SCT in these patientsis not established yet. Overall survival and DFS in our seriesare improved when compared with historical results inpatients treated with chemotherapy alone.4,8-14 A certainselection bias is possible in our series because we onlyincluded the patients who eventually were submitted toSCT. Nevertheless, characteristics of our series were com-parable with those previously reported in infant acuteleukemia, and poor risk factors, such as 11q23 anomalies,CD10Ϫ phenotype, or high WBC count, were frequentlypresent (Table 1). It was the philosophy of the participatingcenters that all (but not only) poor-risk patients would betransplanted. We found 11q23 anomalies in karyotype fromsix patients and evidence of MLL rearrangement was pro-vided by southern blot analysis in two additional cases, fora total of eight 11q23/MLL(ϩ) patients. Interestingly, four
Fig 2. Kaplan-Meier estimated DFS for patients diagnosed with AML
of these eight patients, including two out of four autotrans-
compared with patients with ALL. Differences did not reach statistical significance as determined by the log-rank test.
plants, are long-term disease-free survivors. We are now
collecting molecular data in ongoing patients, so it would
cokinetics,29 the good performance status of most infants,
help to clarify whether the benefit of high-dose chemother-
and the immaturity of their immune systems, which mini-
apy plus SCT could outweigh the prognostic significance of
mizes the risk of GVHD. In the current study, there was not
MLL rearrangement. Lack of expression of CD10 in ALL
any transplant-related mortality. Most of our patients were
patients, which has been associated with poor prognosis, did
conditioned with regimens containing busulfan and cyclo-
not seem to affect outcome in our series, with three out of
phosphamide (BuCy), which have proved to be well toler-
five survivors in both CD10ϩ and CD10Ϫ ALL patients.
ated in infants, avoiding the risk of neuropsychologic
Our good results with autologous SCT put the stress in the
sequelae and other late effects associated with total-body
importance of high-dose chemotherapy more than in pro-
irradiation.17,18 Although toxicity may not be a major
viding a graft-versus-leukemia effect by an allogeneic
problem in infant SCT, relapse remains the first cause of
transplant. It is remarkable that none of our patients devel-
failure. To increase the tumoricidal action of the BuCy
oped extensive chronic GVHD, which could be theoreti-
regimen, we added etoposide in 14 patients; 11 of them
cally associated with a graft-versus-leukemia effect. More-
remain disease-free survivors. Etoposide has been reported
over, previous series of BMT in infant acute leukemia did
as an especially effective agent in AML.30 However, in our
not demonstrate significant differences in outcome between
series, good results with BuCy plus etoposide are not
autologous and allogeneic BMT .17,19,20 Our results also
restricted to myeloid leukemia but are also obtained in ALL
suggest that intensification should be early because a short
infants (Table 1). Other strategies that could be attempted to
interval between CR and SCT was the only significant
reduce the risk of relapse, such as more intensified prepar-
factor associated with a better prognosis in multivariate
ative regimens or posttransplantation immune modula-
analysis. When transplantation was delayed more than 4
tion,19,31,32 need to be assessed in prospective comparative
months from CR1, DFS was dramatically reduced from
92% (SE ϭ 7%) to 38% (SE ϭ 17%). An increased rate of
In conclusion, our study supports the recommendation of
relapse in delayed transplants could be related to emergence
early intensification with autologous or allogeneic SCT
of resistance leukemia phenotypes while on maintenance
rescue for infants with acute leukemia in CR1. An excellent
DFS rate is achieved in patients transplanted within the first
In our experience with SCT in infants, engraftment was
4 months after CR1, with very little transplant-related
good and toxicity was very low. This finding has been
previously reported in other series, suggesting that infants
tolerate the intensification regimens better than older pa-tients.17-20 This may be because of differences in pharma-
We thank Dr Carlos Richard for critical review of the manuscript.
1. Pui C-H, Kane JR, Crist WM: Biology and treatment of infant
8. Pui C-H, Behm FG, Downing JR, et al: 11q23/MLL rearrange-
ment confers a poor prognosis in infants with acute lymphoblastic
2. Pui C-H, Evans WE: Acute lymphoblastic leukemia in infants.
J Clin Oncol 17:438-440, 1999 (editorial)
9. Reaman GH, Sposto R, Sensel MG, et al: Treatment outcome and
3. Basso G, Rondelli R, Covezzoli A, et al: The role of immuno-
prognostic factors for infants with acute lymphoblastic leukemia
phenotype in acute lymphoblastic leukemia of infant age. Leuk Lymph
treated on two consecutive trials of the Children’s Cancer Group. J Clin
4. Sorensen PHB, Chen C-S, Smith FO, et al: Molecular rearrange-
10. Frankel LS, Ochs J, Shuster JJ, et al: Therapeutic trial for infant
ments on the MLL gene are present in most cases of infant acute
acute lymphoblastic leukemia: The Pediatric Oncology Group experi-
myeloid leukemia and are strongly correlated with monocytic or
ence (POG 8493). J Pediatr Hematol/Oncol 19:35-42, 1997
myelomonocytic phenotypes. J Clin Invest 93:429-437, 1994
11. Chessells JM, Eden OB, Bailey CC, et al: Acute lymphoblastic
5. Pui C-H, Kalwinsky DK, Schell MJ, et al: Acute nonlymphoblas-
leukemia in infancy: Experience in MRC UKALL trials—Report from
tic leukemia in infants: Clinical presentation and outcome. J Clin Oncol
the Medical Research Council Working Party on childhood leukemia.
6. Chen C-S, Sorensen PHB, Domer PH, et al: Molecular rearrange-
12. Ferster A, Bertrand Y, Benoit Y, et al: Improved survival for
ments on chromosome 11q23 predominate in infant acute lymphoblas-
acute lymphoblastic leukemia in infancy: The experience of EORTC-
tic leukemia and are associated with specific biologic variables and
Childhood Leukemia Cooperative Group. Br J Haematol 86:284-290,
7. Rubnitz JE, Link MP, Shuster JJ, et al: Frequency and prognostic
13. Silverman LB, McLean TW, Gelber RD, et al: Intensified
significance of HRX rearrangements in infant acute lymphoblastic
therapy for infants with acute lymphoblastic leukemia: Results from
leukemia: A Pediatric Oncology Group study. Blood 84:570-573, 1994
Dana-Farber Cancer Institute Consortium. Cancer 80:2285-2295, 1997
14. Luciano M, Cimino G, Angioni A, et al: A retrospective
24. Glucksberg J, Storb R, Fefer A, et al: Clinical manifestation of
evaluation of infant patients with acute lymphoblastic leukemia treated
GVHD in human recipients of marrow from HLA matched sibling
at a single institution. Haematologica 84:464-465, 1999
15. Pui C-H, Ribeiro RC, Campana D, et al: Prognostic factors in
25. Michel G, Leverger G, Leblanc T, et al: Allogeneic bone
the acute lymphoid and myeloid leukemias of infants. Leukemia
marrow transplantation vs aggressive post-remission chemotherapy
for children with acute myeloid leukemia in first complete remis-
16. Satake N, Maseki N, Nishiyama M, et al: Chromosome abnor-
sion: A prospective study from the French Society of Pediatric
malities and MLL rearrangement in acute myeloid leukemia of infants.
Hematology and Immunology (SHIP). Bone Marrow Transplant
17. Emminger W, Emminger-Schmidmeier W, Haas OA, et al:
26. Tiedemann K, Waters KD, Tauro GP, et al: Results of intensive
Treatment of infant leukemia with busulfan, cyclophosphamide Ϯ
therapy in childhood acute myeloid leukemia, incorporating high-dose
etoposide and bone marrow transplantation. Bone Marrow Transplant
melphalan and autologous bone marrow transplantation in first com-
plete remission. Blood 82:3730-3738, 1993
18. von Bueltzingsloewen A, Esperou-Bourdeau H, Souillet G, et al:
27. Saarinen UM, Mellander L, Nysom K, et al: Allogeneic bone
Allogeneic bone marrow transplantation following a busulfan-based
marrow transplantation in first remission for children with very
conditioning regimen in young children with acute lymphoblastic
high-risk acute lymphoblastic leukemia: A retrospective case-control
leukemia: A Cooperative Study of the Socie´te´ Francaise de Greffe de
study in the Nordic countries—Nordic Society for Pediatric Hematol-
Moelle. Bone Marrow Transplant 16:521-527, 1995
ogy and Oncology (NOPHO). Bone Marrow Transplant 17:357-363,
19. Woolfrey AE, Gooley TA, Sievers EL, et al: Bone marrow
transplantation for children less than 2 years of age with acute
28. Maldonado MS, Dı´az-Heredia C, Badell I, et al: Autologous
myelogenous leukemia or myelodysplastic syndrome. Blood 92:3546-
bone marrow transplantation with monoclonal antibody purged marrow
20. Pirich L, Haut P, Morgan E, et al: Total body irradiation,
for children with acute lymphoblastic leukemia in second remission.
cyclophosphamide and etoposide with stem cell transplant as treatment
Bone Marrow Transplant 22:1043-1047, 1998
for infants with acute lymphocytic leukemia. Med Pediatr Oncol
29. Vassal G, Gouyette A, Hartmann O, et al: Pharmacokinetics of
high-dose busulfan in children. Cancer Chemother Pharmacol 24:386-
21. Reiter A, Schrappe M, Ludwig WD, et al: Chemotherapy in 998
unselected childhood acute lymphoblastic leukemia patients: Results
30. Bishop JF: Etoposide in the treatment of leukemias. Semin
and conclusions of the multi-center trial ALL-BFM 86. Blood 84:3122-
31. Messina C, Zambello R, Rossetti F, et al: Interleukin-2 before
22. Bezanilla JL, Cubells J, Mun˜oz A, et al: Treatment of acute
and/or after autologous bone marrow transplantation for pediatric acute
lymphoblastic leukemia with the Spanish SHOP 89 Protocol: Prelim-
leukemia patients. Bone Marrow Transplant 17:729-735, 1996
inary results. Med Pediatr Oncol 20:407, 1997 (abstr P-63)
32. Atra A, Millar B, Shepherd V, et al: Donor lymphocyte infusion
23. Ortega JJ: PETHEMA protocols in acute lymphoblastic leuke-
for childhood acute lymphoblastic leukemia relapsing after bone
marrow transplantation. Br J Haematol 97:165-168, 1997
Read entire protocol before use. TESTO-EASIA I. INTENDED USE Enzyme Immunoassay for the in vitro quantitative measurement of human Testosterone (TESTO) in serum. II. GENERAL INFORMATION Proprietary name : Catalogue number : Manufactured by : DIAsource ImmunoAssays S.A. Rue de l'Industrie, 8, B-1400 Nivelles, Belgium. For technical assistance or o
BARRY H. SCHWAB, PH.D. EDUCATION Ph.D. Biostatistics, Medical College of Virginia, Richmond, Virginia, 1984 B.A. Statistics, State University of New York, College at Oneonta, 1980 Undergraduate Study Abroad, Tel Aviv University, Israel (1978 – 1979) EMPLOYMENT HISTORY 1984-present Janssen Research & Development, LLC (a J&J company) Vice President, Clinical
 Median age at diagnosis was 7 months (range, 1 to 12 months).
Median age at diagnosis was 7 months (range, 1 to 12 months).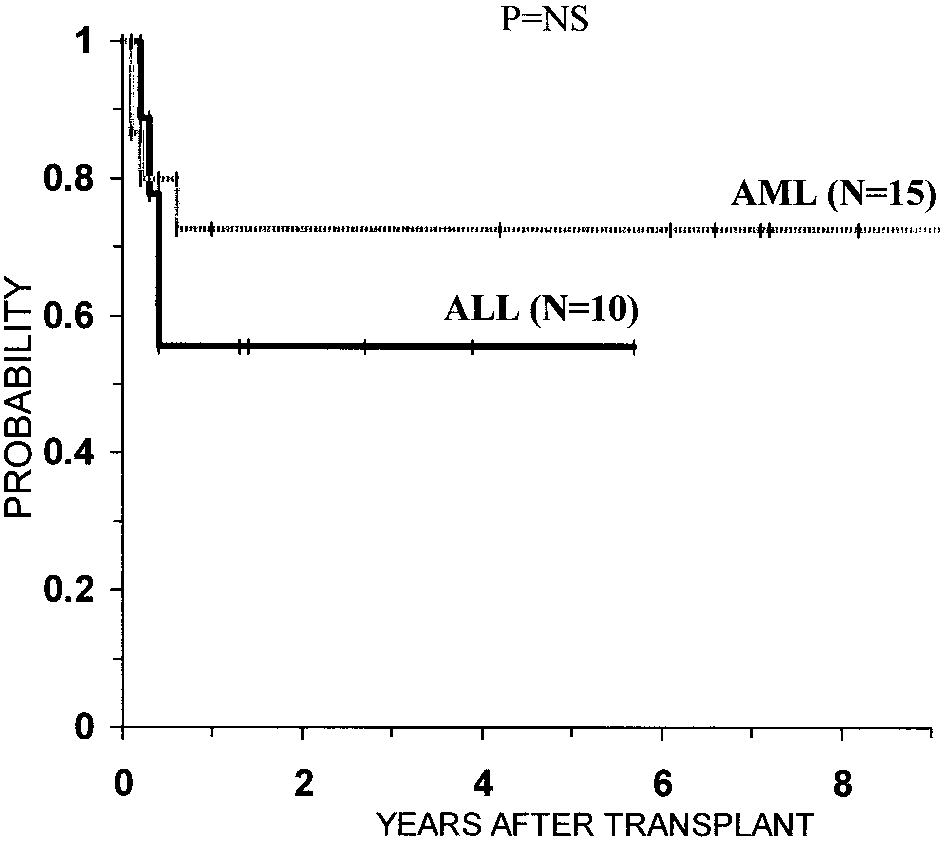
 type, allogeneic SCT, and conditioning regimen. In multi-variate analysis, an interval between CR and SCT of lessthan 4 months was the only significant factor associatedwith greater DFS (P Ͻ .025). In patients transplanted duringthe first 4 months after CR1, DFS is 92% (SE ϭ 8%).
type, allogeneic SCT, and conditioning regimen. In multi-variate analysis, an interval between CR and SCT of lessthan 4 months was the only significant factor associatedwith greater DFS (P Ͻ .025). In patients transplanted duringthe first 4 months after CR1, DFS is 92% (SE ϭ 8%).