Tadalafil entfaltet seine Wirkung über eine selektive Hemmung der PDE5, wodurch die Konzentration von cGMP im glatten Muskelgewebe stabil bleibt. Diese biochemische Modulation resultiert in einer langanhaltenden Relaxation der Gefäßwände. Der Wirkstoff wird nach oraler Einnahme effizient resorbiert, mit einer Bioverfügbarkeit von rund 80 %. Seine Halbwertszeit von bis zu 36 Stunden ist innerhalb dieser Substanzklasse außergewöhnlich. Abgebaut wird er in der Leber, hauptsächlich durch CYP3A4, mit anschließender biliärer Exkretion. Typische unerwünschte Wirkungen entstehen durch eine verstärkte Vasodilatation, etwa Kopfschmerzen oder Flush. Pharmakologisch wird cialis generika vor allem durch die verlängerte Wirkungsdauer charakterisiert.
Dsweb.svc.ops.eu.uu.net
C l i n i c a l C a r e / E d u c a t i o n / N u t r i t i o n O R I G I N A L Comparison of Basal Insulin Added to Oral Agents Versus Twice-Daily Premixed Insulin as Initial Insulin Therapy for Type 2 Diabetes ANS U. JANKA, MD CHRISTINE KLIEBE-FRISCH, PHD ERD PLEWE, MD MATTHIAS A. SCHWEITZER, MD
clinical practice (5,6). In many patients,
ATTHEW C. RIDDLE, MD HANNELE YKI-J¨ARVINEN, MD
insulin treatment is required to achievegood glycemic control (1). OBJECTIVE — To compare the efficacy and safety of adding once-daily basal insulin versus
initiate insulin treatment in type 2 diabetic
switching to twice-daily premixed insulin in type 2 diabetic patients insufficiently controlled by
patients is lacking, and treatment regimens
are known to vary between countries. Sincemost patients with type 2 diabetes are older
RESEARCH DESIGN AND METHODS — In a 24-week, multinational, multicenter,
and physicians’ time is limited, the insulin
open, parallel group clinical trial, 371 insulin-naı¨ve patients with poor glycemic control (fasting
regimen should be easy to apply. However,
blood glucose [FBG] Ն120 mg/dl, HbA 7.5–10.5%) on OADs (sulfonylurea plus metformin)
were randomized to once-daily morning insulin glargine plus glimepiride and metformin
(glargine plus OAD) or to 30% regular/70% human NPH insulin (70/30) twice daily without
monly used, simple regimens for initiating
OADs. Insulin dosage was titrated to target FBG Յ100 mg/dl (both insulins) and predinner
insulin therapy. One approach consists of
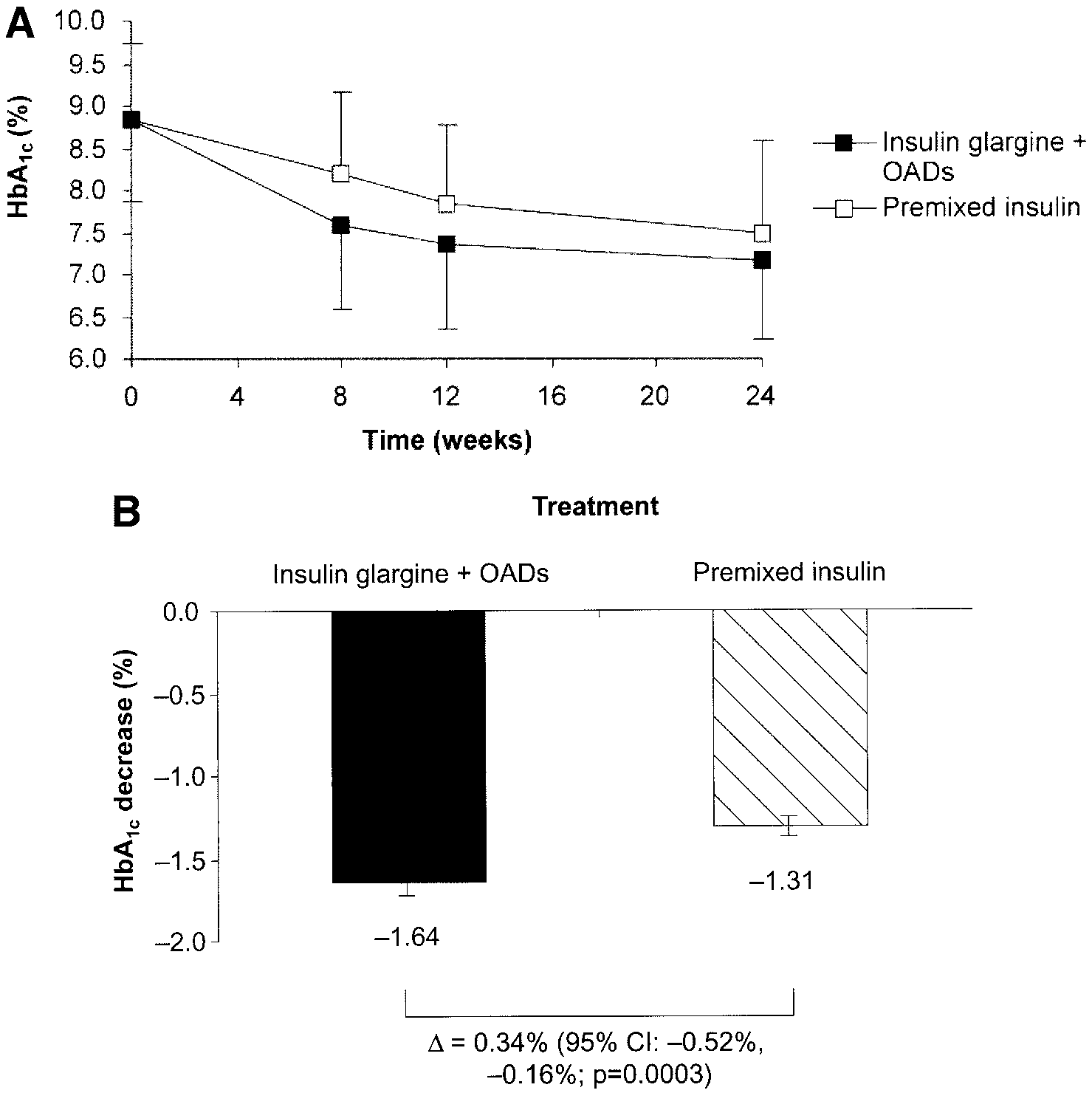
blood glucose Յ100 mg/dl (70/30 only) using a weekly forced-titration algorithm. RESULTS — Mean HbA decrease from baseline was significantly more pronounced (Ϫ1.64 vs.
therapy and initiating two injections of in-
Ϫ1.31%, P ϭ 0.0003), and more patients reached HbA Յ7.0% without confirmed nocturnal
sulin, often premixed insulin containing a
hypoglycemia (45.5 vs. 28.6%, P ϭ 0.0013) with glargine plus OAD than with 70/30. Similarly, FBG
decrease was greater with glargine plus OAD (adjusted mean difference Ϫ17 mg/dl [–0.9 mmol/l],
P Ͻ 0.0001), and more patients reached target FBG Յ100 mg/dl with glargine plus OAD than with
daily. The European Diabetes Policy Group
70/30 (31.6 vs. 15.0%, P ϭ 0.0001). Glargine plus OAD patients had fewer confirmed hypoglycemic
episodes than 70/30 patients (mean 4.07 vs. 9.87/patient-year, P Ͻ 0.0001).
patients with type 2 diabetes, insulin ther-apy should be initiated using premixed in-
CONCLUSIONS — Initiating insulin treatment by adding basal insulin glargine once daily
sulin twice daily. Nearly 40% of insulin-
to glimepiride plus metformin treatment was safer and more effective than beginning twice-dailyinjections of 70/30 and discontinuing OADs in type 2 diabetic patients inadequately controlled
are treated with premixed insulin (7). In-deed, a German study has reported that pre-
Diabetes Care 28:254 –259, 2005
mixed insulin constitutes the majority(Ͼ80%) of insulin usage in patients withtype 1 and type 2 diabetes (8). Another ap-
Theassociationbetweenpoorglyce- with type 1 and type 2 diabetes (1–3); proachincludestheuseofabasalinsulin
cations has been demonstrated in patients
from OADs to twice-daily premixed human70/30 insulin versus adding a once-daily in-
● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ●
jection of basal insulin glargine to priorOADs. The method chosen is, similar to
From 1Zentralkrankenhaus, Bremen-Nord, Bremen, Germany; the 2Division of Endocrinology, Diabetes,and Clinical Nutrition, Oregon Health and Science University, Portland, Oregon; 3Aventis Pharma Deut-
twice-daily premixed insulin, a simple one:
schland, Bad Soden, Germany; and the 4Department of Medicine, University of Helsinki, Helsinki, Finland.
insulin glargine has a 24-h time-action pro-
Address correspondence and reprint requests to Prof. Hans U. Janka, Zentralkrankenhaus, Bremen-Nord,
II Medizinische Abteilung, Hammersbecker Str. 228, 28755 Bremen, Germany. E-mail:
can therefore be administered once daily,
Received for publication 28 July 2004 and accepted in revised form 20 October 2004.
while glimepiride can be taken once daily
H.U.J., M.C.R., and H.Y.-J. have received honoraria and consulting fees from Aventis. Abbreviations: FBG, fasting blood glucose; OAD, oral antidiabetic agent. A table elsewhere in this issue shows conventional and Syste`me International (SI) units and conversion RESEARCH DESIGN AND
2005 by the American Diabetes Association. METHODS — Male or female patients The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be herebymarked “advertisement” in accordance with 18 U.S.C. Section 1734 solely to indicate this fact.
aged 35–75 years with a type 2 diabetes
See accompanying editorial, p. 494.
duration of at least 1 year and treated with
DIABETES CARE, VOLUME 28, NUMBER 2, FEBRUARY 2005
Janka and Associates
formin for at least 1 month were enrolled
the frequency of hypoglycemic events.
at 66 sites in 10 European countries. Fur-
ther inclusion criteria included BMI Յ35
mg/dl (5.6 mmol/l), and the before dinner
levels Ն120 mg/dl (Ն6.7 mmol/l). Exclu-
wise increase of insulin depending on the
sion criteria included any additional use
Statistical analyses were performed on the
glucose Ͼ100 –120 mg/dl, increased by 2
intent-to-treat population, defined as ran-
IU/day; blood glucose Ͼ120 –140 mg/dl,
one injection of insulin. Statistical testing
Ͼ140–160 mg/dl, increased by 6 IU/day; was performed at a significance level of
tained for each participating site. All pa-
ing two-sided 95% CIs were calculated.
with a 1- to 4-week screening phase and a
tests. Statistical analyses were performed
ization schedule stratified by center se-
recovery after oral carbohydrate, intrave-
eligible patients, using a central random-
nous glucose, or glucagon administration.
ization service of the electronic case re-
70/30) predinner blood glucose values, as
groups can be detected with an ␣ error of
0.05 (two sided) and a  error of 0.2 with
RESULTS — A total of 511 patients
dose as before study entry. The dosage of
were screened: 371 patients were eligible
prised the intent-to-treat population.
visit, patients were randomly assigned to
of 4.8 – 6.7%. An eight-point glucose pro-
file (before and 2 h after breakfast, lunch,
and dinner; at bedtime; and at 3:00 A.M.)
fore a visit at baseline and 2, 4, 8, 12, and
24 weeks. The baseline eight-point profile
OAD (3 lost to follow-up and 4 other rea-
twice daily (before breakfast and dinner),
ceiving only glimepiride and metformin.
willing to continue, 5 lack of efficacy, 2
Adverse events were noted by the investi-
gator at every visit or telephone contact.
injected using Optipen 1E for insulinglargine and NovoPen for premixed insu-
lin. The starting dose for insulin glargine
mixed insulin, 10 IU before breakfast and
10 IU before dinner. These starting doses
could be lowered if considered clinically
to 7.49 Ϯ 1.09% with 70/30 (Fig. 1A).
Յ100 mg/dl (Յ5.6 mmol/l), proportion Mean adjusted HbA1c improvement was
doses were adjusted by a forced titration
Յ7.0% with no nocturnal hypoglycemia, [95% CI Ϫ1.51 to Ϫ1.78]) than with
for 8 weeks and at 2-week intervals there-
after for both groups, according to daily
self-monitored capillary whole blood glu-
ence of Ϫ0.34% (Ϫ0.52 to Ϫ0.16%, P ϭ
DIABETES CARE, VOLUME 28, NUMBER 2, FEBRUARY 2005
Glargine plus oral agents vs. premixed insulin Table 1—Baseline demographics and characteristics of the study population
mg/dl (9.5 to 6.4 mmol/l) with glargineplus OAD and from 172 to 133 mg/dl (9.6to 7.4 mmol/l) with 70/30. Improvement
Ϫ24 to Ϫ10 mg/dl [–1.3 to Ϫ0.6 mmol/
l], P Ͻ 0.0001). A greater proportion of
Data are means Ϯ SD unless otherwise indicated. OAD refers to sulfonylurea plus metformin.
blood glucose level improved from 182 to137 mg/dl (10.1 to 7.6 mmol/l) in the
0.0003) significantly favored the glargine
the 70/30 group (P Ͻ 0.0001 for be-
confirmed nocturnal hypoglycemia (P ϭ
70/30 group (P ϭ 0.0596 for the be-
tween-treatment difference). Significantly
weeks (mean Ϯ SD) in insulin glargineplus glimepiride and metformin (insulinglargine ϩ OADs) and premixed insulintreatment groups. B: Improvement inHbAbaseline [before insulin initiation] to endpoint Ϯ SE).
DIABETES CARE, VOLUME 28, NUMBER 2, FEBRUARY 2005
Janka and Associates
Figure 2—Twenty-four– hour eight-point blood glucose profiles at baseline (before insulin initiation) and end point in insulin glargine plusglimepiride and metformin (insulin glargine ϩ OADs) and premixed insulin treatment groups (*P Ͻ 0.05 for treatment comparison of changes frombaseline to end point).
at the fasting, postlunch, dinner, postdin-
ner, and 3:00 A.M. time points (Fig. 2).
was 1.4 Ϯ 3.4 and 2.1 Ϯ 4.2 kg, respec-
Insulin dose increased over the study du-
tively (P ϭ 0.0805 for between-group
CONCLUSIONS — These results
show that in patients with type 2 diabetes
dose of 9.9 Ϯ 2.6 to 28.2 Ϯ 15.2 IU at end
poorly controlled on oral therapy, adding
point for insulin glargine. The prebreak-
a single injection of insulin glargine to
from the mean starting dose of 10.3 Ϯ 2.5
ilar; 89 patients (50.3%) in the glargine
more effective glycemic control than stop-
31.0 Ϯ 16.1 IU at end point, resulting in
respiratory disorders (16%), nervous sys-
tem disorders (10%), and gastrointestinal
patients on 70/30 insulin achieved target
per patient-year and the number of events
One hundred nine patients (61.6%) re-ceiving glargine plus OAD and 127 pa-
Table 2—Mean number of confirmed* hypoglycemic events per patient-years
t i e n t s ( 6 7 . 2 % ) r e c e i v i n g 7 0 / 3 0experienced at least one hypoglycemicevent (P ϭ 0.2838). During treatment,
events, expressed as episodes per patient-
years, was ϳ50% lower with glargine plus
symptomatic, and nocturnal categories(Table 2). Severe hypoglycemia was very
*Hypoglycemia was confirmed by blood glucose Ͻ60 mg/dl (3.3 mmol/l). †Severe hypoglycemia wasdefined as symptoms consistent with hypoglycemia that required the assistance of another person and were
associated with either a blood glucose level Ͻ36 mg/dl (Ͻ2.0 mmol/l) or prompt recovery after oral
carbohydrate or intravenous glucose or glucagon.
DIABETES CARE, VOLUME 28, NUMBER 2, FEBRUARY 2005
Glargine plus oral agents vs. premixed insulin
The relatively low total daily insulin dose
2. Ohkubo Y, Kishikawa H, Araki E, Miyata
cemia with the basal insulin regimen is of
particular interest because fear of hypo-
glycemia remains one of the key obstacles
therapy prevents the progression ofdiabetic microvascular complications in
to both initiating and optimizing insulin
titration to achieve target HbA1c in more
therapy (11–13). The difficulty of manag-
patients. Even so, some patients will re-
ing multiple injections and the associated
quire additional prandial injections of in-
prospective 6-year study. Diabetes Res Clin
sulin to reach the Յ7% HbA1c target.
3. The Diabetes Control and Complications
strated that, for patients with type 2 dia-
regimen in this study required only a sin-
cations Trial. Diabetes 45:1289 –1298,1996
4. Stratton IM, Adler AI, Neil HA, Matthews
than starting twice-daily injections of pre-
vascular complications of type 2 diabetes
regimens for initiating insulin rather than
Acknowledgments — This study was sup-
5. European Diabetes Policy Group 1999: A
Investigators: Austria: W. Fortunat, A.
desktop guide to type 2 diabetes mellitus.
Holler, R. Prager, J. Thomas, and T. Wascher;
Finland: H. Yki-Ja¨rvinen; France: J.F. Blickle,
J.M. Brun, M. Rodier, and B. Schmitt; Ger-
dards of medical care for patients with di-
therapy with premixed insulin (15–17).
many: P. Brommer, K. Busch, H. Dancygier,
abetes mellitus (Position Statement).
E.M. Fach, T. Feldmann, A. Fiesselmann, G.
Garanin, J. Grosskopf, J. Habbig, T. Hampel,
7. Koivisto V, Tuominen J, Ebeling P: Lispro
H. Herrmann, H.U. Janka, K.A. Jahnke, V.
Jung, M. Kiper, C. Klein, D. Klein, V. Koch, K.
2 diabetic patients. Diabetes Care 22:459 –
pared with 70/30 insulin alone. In clinical
Langer, E. Lohr, C. Marck, H.J. Marks, P.
Mayr, S. Maxeiner, O. Mueller, F. Odemar, A.
8. Hauner H, Koster L, von Ferber L: Preva-
Pfuetzner, H. Pitule, H. Samer, G. Scholz, A.
Sterzing, H.J. Strotmann, J. von Huebbenet, J.
1998 –2001. Dtsch Med Wochenschr 128:
Wachter, and U. Wendisch; Italy: A. Civarella,
pected to improve the effectiveness of this
G. Riccardi, G. Rosti, G. Seghieri, and G.
9. Lepore M, Pampanelli S, Fanelli C, Por-
Vespasiani; the Netherlands: R. van Doorn, L.
cellati F, Bartocci L, Di Vincenzo A, Cor-
regarding the initiation of insulin therapy
Lieverse, and W. Venekamp; Spain: B.F. Go-
in patients with type 2 diabetes. The cur-
mis, C.F. Hawkins, R.G. Mayor, A. Novials,
and J. Zurro Hernandez; Sweden: B. Lindgren
ics of subcutaneous injection of long-act-
and M. Palmer; Switzerland: P. Gerber; U.K.:
R. Bilous, D. Gordon, C.M. Kesson, M. Samp-
insulin, and ultralente human insulin and
Study team: M. Herbold, C. Kliebe-Frisch,
sulin lispro. Diabetes 49:2142–2148,
S. Krull, A. Loehr, W. Messer, A. Mueller, H.
clude addressing the benefit of 70/30 in-
Nortmeyer, J. Peiker, T. Schlink, and N. Tjia.
sented in abstract form [Diabetes 53 (Suppl.2):
action profile of the long-acting insulin
formin on the results obtained in the in-
A130, 2004 and Diabetelogia 47 (Suppl. 1):
sulin glargine–treated group. In addition,
A269, 2004] and presented as posters at the
with those of NPH insulin and placebo.
American Diabetes Association Scientific Ses-
Diabetes Care 23:644 – 649, 2000
sions 2004 and the European Association for
11. Korythowski M: When oral agents fail:
the Study of Diabetes Congress 2004.
practical barriers to starting insulin. Int JObes Relat Metab Disord 26:S18 –S24,
ment with all of these regimens, including
References
12. Johnson R, Hauber B, Bolinder B: Trade-
glycemia in different patient types: results
stract). Diabetes 52 (Suppl. 1):A264, 2003
complications in patients with type 2 di-
one-half of patients in the glargine plus
abetes (UKPDS 33). Lancet 352:837– 853,
DIABETES CARE, VOLUME 28, NUMBER 2, FEBRUARY 2005
Janka and Associates
Lahti J, Marjanen T, Niskanen L, Rajala S,
insulin regimens in elderly patients with
basal insulin: can glargine reduce barrier
Ryysy L, Salo S, Seppa¨la¨ P, Tulokas T, Vi-
NIDDM. Diabetes Care 19:1326 –1332,
to target attainment? (Abstract). Diabetes
ikari J, Karjalainen J, Taskinen M-R: Com-
parison of insulin regimens in patients with
non-insulin-dependent diabetes mellitus. N Engl J Med 327:1426 –1433, 1992
progress to date. Am J Med 113 (Suppl.
16. Wolffenbuttel BH, Sels JP, Rondas-Col-
control but lower weight gain than insulin
twice daily in patients with type 2 diabe-
15. Yki-Ja¨rvinen H, Kauppila M, Kujansuu E,
tes. Diabetes Metab 28:272–277, 2002
DIABETES CARE, VOLUME 28, NUMBER 2, FEBRUARY 2005
Untersuchungsbericht über das Attentat auf Oberst Estermann (aus: «Der Exgardist», Nr. 67/1999, S. 94–101, und Nr. 68/2000, S. 130–136) Aufschluss über die Untersuchung wegen des Todes des neuernannten Kommandanten der Päpstlichen Schweizergarde, Oberst Alois Estermann, seiner Ehefrau Gladys Meza Romero und des Vizekorporals der Garde, Cédric Tornay, eingetreten am Abend des
Web: www.spinepainbegone.com | Phone: 210.251.3671 | Fax: 210.615.8606 PRE-OP CHECKLIST & INFORMATION >> BEFORE SURGERY If you smoke, it is advised that you quit as far before surgery as you can. Your physician can assist you with prescriptions for this. You may be asked to register at the hospital or surgery center ahead of time. Avoid drinking alcohol (
 Glargine plus oral agents vs. premixed insulin
Glargine plus oral agents vs. premixed insulin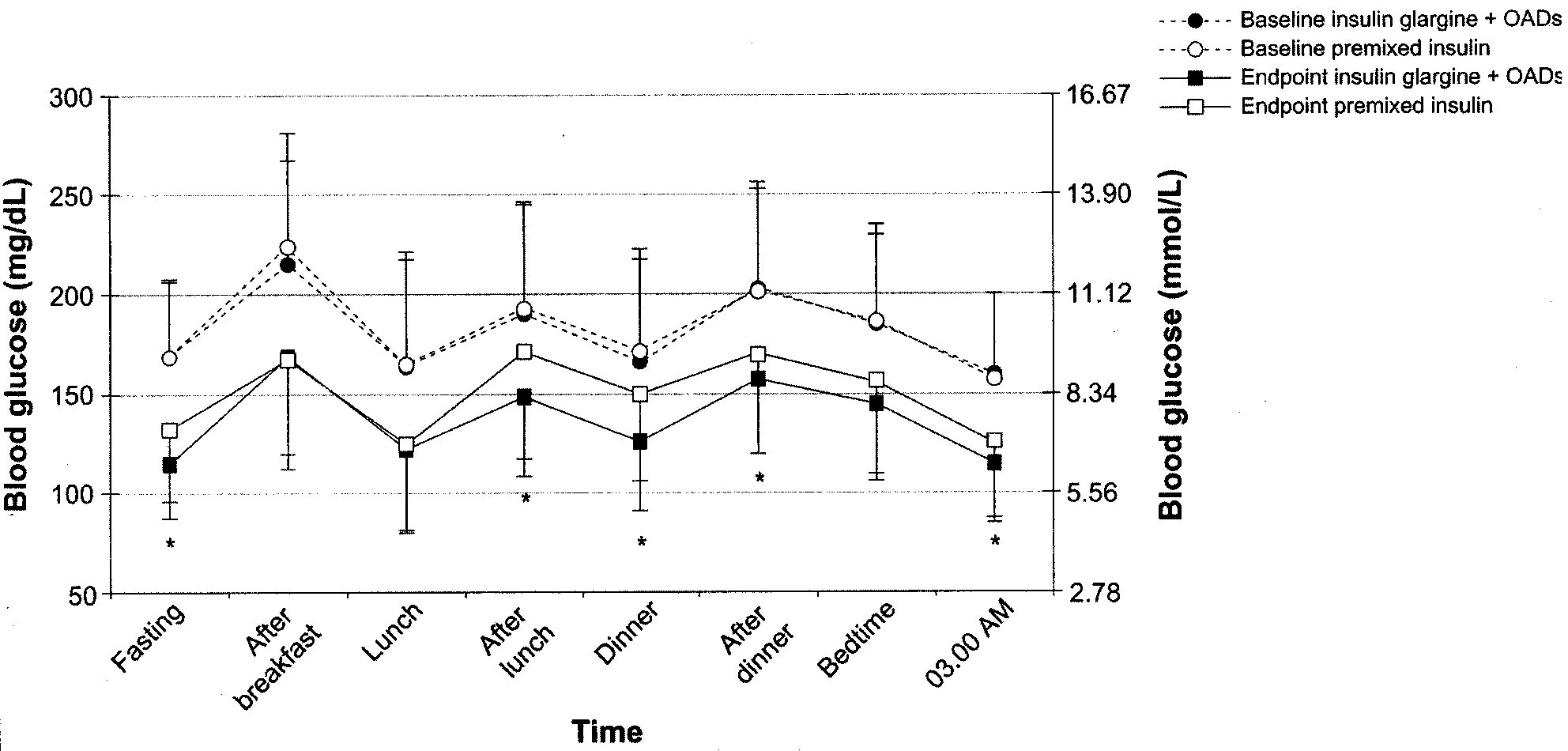 Janka and Associates
Janka and Associates