Tadalafil entfaltet seine Wirkung über eine selektive Hemmung der PDE5, wodurch die Konzentration von cGMP im glatten Muskelgewebe stabil bleibt. Diese biochemische Modulation resultiert in einer langanhaltenden Relaxation der Gefäßwände. Der Wirkstoff wird nach oraler Einnahme effizient resorbiert, mit einer Bioverfügbarkeit von rund 80 %. Seine Halbwertszeit von bis zu 36 Stunden ist innerhalb dieser Substanzklasse außergewöhnlich. Abgebaut wird er in der Leber, hauptsächlich durch CYP3A4, mit anschließender biliärer Exkretion. Typische unerwünschte Wirkungen entstehen durch eine verstärkte Vasodilatation, etwa Kopfschmerzen oder Flush. Pharmakologisch wird cialis generika vor allem durch die verlängerte Wirkungsdauer charakterisiert.
Ejbo_vol9_no2.indd
EJBO Electronic Journal of Business Ethics and Organization Studies
Introduction
equal relationship with their physicians.
This paper reviews current marketing On the other hand action groups such as
Abstract
practices in the pharmaceutical sector, the U.S. Public Citizen’s Health Research
oriented promotion. It presents examples tend that there is no evidence that such
of marketing practices and their impact advertising improves health care.
identifies negative impacts of these prac-
area to engage with, given that Big Phar-
ing, disease mongering and escalating ing example. They engage in multi-mil-
costs. It goes on to argue the need for an lion dollar marketing campaigns, use all
tice for marketers in the pharmaceutical advertising, to below the line spend on
sector and a greater degree of consumer measures such as the engagement of key
education for both end-users and those opinion leaders. Many billions of dollars
tecting not alone their branded products
The context Keywords Pharmaceutical marketing methods, How are drugs promoted?
entitled“time to untangle doctors from a so-called block-buster drug is current-
drug companies”(Moynihan 2003). The ly estimated at $895 million (EFPIA,
theme was relationship between the 2002). Obviously firms who spend that
kind of money need to recoup their costs.
cal profession in Europe, in conjunction that Big Pharma under pressure. It needs
with many social movements, has begun to expand sales of blockbuster drugs
since there are fewer drugs in pipeline. In
ness of current relationships between order to sustain current levels of growth,
Big Pharma and the health sector. This firms would need to introduce one new
is occurring in the context of legal actions product each year that would sell $4.9
around corrupt sales practices in Europe million for each 1 to 1.5 per cent it has
such as those against GlaxoSmithKline of the world pharmaceutical market. “A
aly (Turone 2003), and the major action Glaxo Wellcome/Smith KlineBeecham
against TAP Pharmaceutical Products, needs three to seven products each year,
Inc in the United States which resulted in while one the size of Astra Zeneca needs
a $875 million dollar settlement in 2001 two to four products each year. The prob-
lem is that research productivity is fail-
This debate is already very strong in ing. None of the major companies is close
the United States where it has further to the target.” (Horrobin 2000)
between Big Pharma and consumers. the nature of the marketing mission is
This is in part because of US practice of different. There are essentially two cat-
allowing direct- to-consumer advertising egories of drugs: self-medication or over
(DTCA) of prescription drugs. Industry the counter (OTC) drugs, and prescrip-
tion drugs - sometimes referred to as eth-
tical industry argue that such advertising 1997). OTC drugs are promoted directly
(properly regulated) allows consumers to consumers as well as physicians and
to inform and educate themselves about other healthcare professionals and range
EJBO Electronic Journal of Business Ethics and Organization Studies
from analgesics such as paracetamol to anti-histamines. What broadcast DTCA of these drugs has resulted in increased “pull”
is categorized as OTC varies from country to country and is de-
from consumers. In both the United States and New Zealand
pendent on the local legislative framework – usually a national DTCA of prescription drugs occurs with considerable effect, as
medicines authority, so for example in the United States some will be discussed below. A further source of ‘indirect’ pull has
been the impact of the Internet on pharmaceutical promotion,
Corstjens (1991) identifies four main buying parties for pre-
1. Prescriber – prescribing rights vary internationally and
this category may include doctors, dentists, pharmacists, nurses Direct to consumer promotion – creating direct pull
2. Influencer – hospitals, nurses, professors, reimburse-
In August 1997 the US FDA made significant changes in the
regulations for broadcast DTCA of prescription drugs. Prior to
4. Financier – partly patient, partly government or third 1997 DTCA had to include the entire brief prescribing infor-
party (varies by country), managed health care organization mation which meant that about 30 seconds out of a 60 second
(hospitals, Health Maintenance Organisations etc.)
advertisement would consist of fine print scrolling across the
The majority of Big Pharma’s marketing budget is targeted screen. In 1997 the FDA dropped this requirement and said that
at doctors and others with prescribing power, who are effective-
DTCA had to mention the major side-effects, and also provide
ly the gatekeepers to drug sales. In 2002 the Canadian Medi-
other ways that consumers could get more information about
cal Association Journal estimated some US$19 billion is spent the drug (e.g. give a web site, a 1-800 number or refer to a print
by Big Pharma annually in promoting drugs to doctors in the ad for the same product which contained the same information)
United States alone. The methods used will be discussed later and tell consumers to consult their doctors/pharmacists. In the
four-year period from 1996 to 2000 promotional spend direct
In the European Union only OTC drugs are promoted di-
to consumer within the United States tripled (from $791 mil-
rectly to consumers. Examples include analgesic preparations lion dollars to $2.5 billion dollars, New England Medical Jour-
and some ailment-specific drugs such as the Schering Plough nal 14/2/02). New Zealand is the only other developed coun-
blockbuster Clarityn - a hayfever remedy. In 1998 Schering try that allows DTCA of prescription drugs. Burton (2003)
Plough spent $186 million promoting Clarityn, and as a result details a report by academics from all of New Zealand’s medical
saw a half a billion dollar increase in sales year on year to achieve schools which recommended that the practice be discontinued.
annual sales of $1.9 billion, (Maguire 1999).
This report, based on a survey of all general practitioner doctors
In the United States all drugs may be promoted to consum-
in New Zealand, found that seventy five per cent of respondents
ers, but in practice direct to consumer advertising focuses on believed DTCA to be negative with patients frequently request-
OTC and common-ailment targeted prescription drugs. There ing drugs that were inappropriate to them. On the other hand
are other more limited application drugs for less common dis-
in New Zealand drug advertising is not monitored by a state
eases that are only promoted to health care professionals, and agency (whereas it is in the United States). The pharmaceu-
hospital and organizational formulary committees (such as tical and advertising industries are self-regulating. This leads
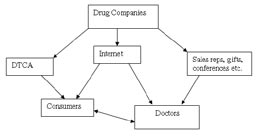
HMO formulary committees). The drug marketing process to a less than ideal situation where only a small percentage of
can be described by the model below in Figure 1, which shows the televised pharmaceutical advertisements are compliant with
the information flow from drug companies, both to consumers the New Zealand Medicines Act regulations, which ostensibly
and doctors. It also shows the power that consumers, informed control for information on contra-indications, and safety and
by DTCA and the Internet, have in “pulling” prescription drugs quality of medicines (pharmacovigilance). Effects of DTCA on consumers
Flynn (1999) argues that DTCA makes consumers better
informed and more sophisticated. In his view consumers are
enabled, through DTCA, to better understand the market for
drugs and the therapeutic options available to them. This view
is also shared by Calfee (2002), who argues that consumers can
engage in more equitable relationships with health care provid-
ers and become partners in their own health care as a result
of DTCA. Mintzes et al (2002) found that consumers pulled
prescription drugs through the system, going to physicians with
Figure 1. Pharmaceutical marketing process.
requests for medications that they had learnt of through adver-
tisements. Their research showed that patients normally got
Creating the Pull – Directly and Indirectly:
positive responses to requests for prescriptions. Their research
also showed that physicians were influenced in their choice of
Historically promotion for prescription drugs occurred only drugs and might otherwise have prescribed different drugs.
from manufacturer to prescriber so that physicians and oth-
Maguire (1999) likewise suggests that American physicians
ers with prescribing powers were the gatekeepers to eventual are being asked to ‘rubber stamp’ self-diagnoses and self-pre-
drug sales. The promotion strategies therefore were all essen-
scriptions by patients. Citing a study by Prevention magazine
tially “push” focused. However the decision in 1997 by the US of the previous year she suggests that 15.1 million U.S. consum-
Food and Drugs Administration (FDA) to relax restrictions on ers asked their physician for a medication they saw advertised,
EJBO Electronic Journal of Business Ethics and Organization Studies
and that physicians honoured those requests eighty percent of The United Kingdom Medicines Control Agency subsequently
the time, which translates into 12.1 million prescriptions gen-
stopped this initiative citing it as unlawful promotion. However
erated by advertising. Further evidence of the effectiveness of Herxheimer (2003) points out that in the absence of adequate
DTCA is the fact that visits to doctors for conditions covered in independent funding patients organisations and lobbying
advertising campaigns rose 263 per cent in the first nine months groups are likely to continue to accept funding from pharmaceu-
of 1998, in comparison to a general 2 per cent rise in visits to tical companies despite the clear ethical issues. He gives as ex-
doctors. Lexchin and Mintzes (2002) examining the relation-
amples the International Alliance of Patient Organisations and
ship between DTCA and prescribing practices find that DTCA the Global Alliance of Mental Health Illness Advocacy which
does affect doctors’ prescribing patterns, which they suggest are both highly visible and linked financially to Big Pharma.
is not always a positive development. They give as an example
Medawar (2002) quotes the Chairman of the Danish Mi-
General Motors’ 1999 internal study of the prescription of the graine Association who suggests that patient organizations are
gastrointestinal drug Prilosec (the second most heavily DTC becoming more sophisticated in their interactions with Big
promoted drug in 1999) to its employees. GM found that 92% Pharma and may become hardened to this form of below the
of those who received a prescription for Prilosec had not received line promotion. The chairman tells of the association’s experi-
a previous prescription or even consulted a doctor previously ences when it refused to take industry assistance in its activities
for gastrointestinal problems. Most received Prilosec as a first – magazines, lectures and administration. “the industry, gen-
line drug without first trying other cheaper and less intensive erally assisted by the research doctors, literally created a new
treatments. Lexchin and Mintzes argue that this is evidence that patient organization as a substitute for the Migraine Associa-
DTC has impacted on prescribing patterns, effectively creating tion in 1996. This was a bit too blatant to be generally accepted
consumer pull for in some cases inappropriate therapies.
among informed patients and opinion makers, but only because
we did not accept the situation gracefully and made the press
aware of our situation. …. Luckily we have a growing awareness
Creating pull indirectly
Medawar points out that Big Pharma have been successful
Increasingly consumer pull for drugs is being created indi-
in presenting their concerns to reach consumers directly as a
rectly also by Internet promotion, and perhaps more question-
consumer rights issue, and a potential positive contribution to
ably by partnerships with patient support groups.
national health profiles. He suggests that Big Pharma is “gradu-
ally shifting the core of its business away from the unpredictable
Consumers are able to purchase all kinds of prescription and increasingly expensive task of creating drugs and toward the
drugs online often without need for a prior prescription. Re-
search conducted by Bloom (1999) showed that most Internet
pharmacies provide poor quality information, fail to have ad-
equate safeguards to ensure medicines are dispensed correctly, The Push Strategy: Promotion to Physicians and
and also charge more for both products and services. Smith health-care professionals
(2003), referring to an Australian study, found that online
pharmacies often lacked important information about contra-
“Despite the boom in consumer ads, doctors are still king”
indications for medications available on their sites. However Maguire (1999)
even if one sets aside the impact of Internet pharmacies, on the
However enormous the implications of DTCA of drugs
basis that the additional costs may put them outside the reach and the budgets devoted to this, the issue of physician targeted
of consumer, the Internet has also offered Big Pharma a largely promotion is significantly greater on all fronts, both financially
unregulated way to reach the consumer directly – through com-
and in terms of eventual outcomes. Komesaroff and Kerridge
pany websites. For example, if one searches the Lilly blockbuster (2002) state that promotion and marketing to doctors makes
Prozac on the internet and goes to the manufacturer’s website up a quarter to a third of their annual budgets “… totaling more
one can take self-diagnostic tests which allow the possibility for than US$11 billion each year in the United States alone).There
the internet user to self-diagnose depression, even if the site in-
are no comprehensive figures available, but it is estimated that, of
this, about US$3 billion is spent on advertising and US$5billion
on sales representatives, while expenditure per physician is be-
lieved to be over US$8000.” As mentioned earlier in this article
Using patient support groups
the Canadian Medical Association Journal in 2002 estimated
the US promotional spend to be even higher at approximately
Jeffries (2000) writing about the Association of the British $19 billion dollars. This activity includes advertising, gift giv-
Pharmaceutical industry’s strategy for the future of its mem-
ing and support for medically related activities such as travel to
bers “The ABPI battle plan is to employ ground troops in the meetings and support for conferences.
form of patient support groups, sympathetic medical opinion
Why do firms spend so much on promotion to doctors? Es-
and healthcare professionals – known as stakeholders” which sentially because they rightly see that doctors are the gatekeep-
will lead the debate on the informed patient issue”. This tactic is ers to the success of individual brands. To quote Barnes (2003)
well illustrated by the following quote from Boseley (1999) “A “Prescribing ‘events’ such as a physician swapping one brand for
pharmaceutical company will tomorrow break new ground by another …. Can make or break a brand’s success.”
encouraging the public to demand that the NHS pay to make
Doctor-targeted promotion takes a variety of forms:
available one of its drugs. The campaign, Action for Access, is
Gifts, such as free samples, small stationery (Riccardi
funded by Biogen and organized by a PR company on its behalf. 2002), travel to conferences and educational events, and, some
It will urge multiple sclerosis sufferers to demand their health argue, cash (Medical Marketing & Media 2003, Prawirosujanto
authorities agree to prescribe beta-interferon on the NHS, a 2001, Strout, 2001)
very expensive drug, which can help some sufferers, but not all”.
Sponsorship of conferences and educational events
EJBO Electronic Journal of Business Ethics and Organization Studies
(Moynihan 2003, Hayes et al 1990, Komesarroff and Kerridge advantages over existing listed medicines
The use of key opinion leaders – i.e. senior clinicians
and medical educators as speakers at learned conferences Lerer
Prescribing of fewer generics and more expensive new
medications at no demonstrated advantage.
Funding of medical journals through advertising.
Komesaroff and Kerridge (2002) also point to the many
Pharmaceutical companies use medical journals to advertise studies that indicate the advertising rather than clinical evidence
their products, and frequently advertising revenue is the only alone affects clinical decision-making. They cite Peay and Peay
source of funding of these journals, which are often sent free to (1988) who found that physicians exposed to advertising are
doctors. Smith (2003), the editor of the British Medical Journal, more likely to accept commercial evidence, rather than well-es-
writes thus of advertising by Big Pharma “To attract advertising tablished scientific views.
these publications have to be read by the doctors whom the ad-
As Lexchin and Mintzes (2002) argue, if advertising re-
vertisers want to reach. So the free publications work hard at sults in these negative outcomes with physicians who are more
making themselves attractive, relevant, interesting, and easy to knowledgeable about drugs and can more easily access objective
read – in contrast to journals, which are often delivering com-
information, “how realistic is it to believe that consumers will be
plex, difficult to read material of limited relevance.” Davidoff et positively affected?”
al 2001 write of a decision among the editors of some of the
world’s largest medical journals to adopt a common policy of
disclosure of information about the source and validity of arti-
Why should this we be concerned with this?
cles submitted for publication, and possible conflicts of interest.
Hence, for example, contributors to the British Medical Journal
There are a number of key reasons for concern about the im-
must disclose any potential conflicts of interest that might arise. pact of pharmaceutical companies’ marketing strategies. These
This policy does not however apply in the non-medical press include:
and women’s magazines, and many of the world’s broadsheets
The fact that drug promotion is often misleading
carry thinly-veiled info-mercials for medical conditions, such as
Revill’s coverage of female testosterone deficiency in the United
The increasing costs of drugs within national health
Kingdom national newspaper The Observer in Jan 2003.
“ We doctors are shamelessly manipulated by drug compa-
New drugs are the ones most heavily promoted and
nies in all sorts of ways. .the methods cover the whole spectrum these are the ones with the least well-understood safety pro-
from subliminal to brazen, from little pens that don’t work to files. Drug promotion often misleading Doctors’ responses to Big Pharma promotion
Much drug advertising is misleading. A U.S. congressional
Doctors are obviously not undiscerning recipients of adver-
inquiry reported that from August 1997 to August 2002 the
tising and other forms of promotion. Smith (2003) says “Your FDA issued 88 letters accusing drug companies of advertising
opinion may not be bought, but it seems rude to say critical violations. In many cases companies overstated the effectiveness
things about people who have hosted you so well.” He goes of the drug or minimised its risks (Gottlieb 2002). Aitken and
on to say that the easy dichotomy of pharmaceutical giants as Holt (2000) found that the FDA filed violation notices for one
villains and doctors as innocent victims is over-simplifying the in four products supported by DTCA. As discussed earlier the
situation. Clearly doctors need to use drugs in order to deliver instance of non-compliance with medicines board’s require-
their services, and it is also reasonable that firms should be al-
ments for accuracy is even higher in New Zealand. PHAR-
lowed to promote their products. “But surely doctors should be MAC, the New Zealand government’s drug purchasing agency,
looking also to independent sources of information, and how has raised considerable concerns about the impact of DTCA
did we reach a point where so many doctors won’t attend an saying that consumers interpret the existence of DTCA as gov-
educational meeting unless it’s accompanied by free food and a ernment approval of advertised brands, which leads them to
discount potentially important risk information.
Separate studies by McInney, Scheidermeyer, Lurie et al
(1990), Banks and Mainour (1992) and Chren, Landefeld and
Murray (1989) all found that there was a strong correlation Misleading advertising can lead to unrealistic
between doctors’ tendencies to recommend drugs and their re-
expectations
ceipt of gifts/sponsorship/ non-related payment etc. Studies by
Wazana (2000), Chren et al (1989) and Thomson, Craig and
There are many instances of inappropriate drug advertising.
Barnham (1994) all show that gifts impact on doctors’ prescrib-
Healthy Skepticism New Zealand (HSNZ), a publication of
ing practices. Wazana (2000) examined 29 empirical studies of the Medical Lobby for Appropriate Marketing, focused on some
the impact of interactions between the medical profession and of the issues relating to promotion of Viagra in June 2000. They
Big Pharma. Synthesising these findings certain negative out-
found that the product claims made were in many cases inap-
comes were found to be associated with interactions with the propriate since they did not offer enough clarity. The Pfizer ad
in New Zealand was as follows “About 52% of men aged 40 to
Inability to identify inaccurate claims about medica-
70 are affected by erectile dysfunction ….In clinical trials 78%
of men reported improvements in their erections. So Viagra will
Rapid adoption and prescription of new drugs
work in about 4 out of 5 men.” HSNZ took issue with the ad on
Formulary requests for medications without important the following grounds:
EJBO Electronic Journal of Business Ethics and Organization Studies
The 52% figure was inaccurate and misleading and had by Medawar (2001).
no basis in fact. It was rather the extrapolation of a very limited
These views are directly at odds with the reality of pharma-
but favourable related clinical trial.
ceutical industry practices such as that of increasing brand pen-
This claim could affect men with confidence rather etration through identifying new ailments that may be treated
than medical problems – they argue that “exaggerating the se-
by existing drugs (thus extending the brand’s target markets and
verity and/or frequency of conditions to expand markets has potentially its sales). This is well illustrated by U.S. advertise-
ments promoting the Pfizer anti-depressant Zoloft as a poten-
That “will work” was misleading since it might give the tial solution to PMDD – pre-menstrual dysphoric disorder,
impression that Viagra would “work well enough to enable suc-
which has symptoms not that dissimilar to pre-menstrual syn-
cessful sex” which was not always true. They point to clinical drome (PMS). Similarly the BBC reported a story in Sep 2000
studies which suggest that the success rate of Viagra was in fact of the propensity of U.K. doctors to prescribe Proxac for PMS
They also point out that efficacy in the real world may
not equate to the efficacy reported in clinical trials because of
halo effects created by enthusiastic specialists. Ever-increasing costs
They suggest that the ad is “a fallacy of over-simplifi-
cation” which doesn’t convey that improvement in dysfunction
Ess, Schneeweiss and Szucs (2003) show that expenditures
may not result in successful sex, and is a function of the degree on drugs have grown faster than the gross national product in all
European countries, as in the United States. They identify the
While patients might be very disappointed because of un-
various methods by which member states attempt to control.
realistic expectations based on advertisements, these are not as Increased controls on costs – by price fixing, or drug budgetting
serious as what HSNZ see as the irresponsible downplaying of . This parallels the United States where Health Maintenance
risks. In a much smaller font on the ad the following three sen-
Organisations and company health schemes already limit their
tences are printed in bold: “You must not take Viagra if you are formularies and will not pay for certain drugs (this is not to sug-
using any nitrate medication including amyl nitrate (poppers). gest formulary limitation is in itself wholly negative, it depends
It may lead to a severe drop in your blood pressure, that may be on the selection criteria used to make decisions on whether to
difficult to treat. As sexual activity may be a strain on your heart include or exlude drugs).
your doctor will need to check whether you are fit enough to use
For example both the Californian Health Maintenance Or-
Viagra.” HSNZ take issue with this warning because they feel it ganisation Kaiser Permanente, and the NHS in Britain refuse
is inadequate, because the use of technical terms such as nitrate to reimburse patients for Viagra. Moynihan (2003) also points
medication, rather than brand names may mean that those po-
out that costs have spiraled for drugs, vastly exceeding national
tentially at risk do not recognize the risks; “readers may not real-
rates of inflation. Echoing Medawar’s (2002) point, it would
ize that the ‘severe drop in blood pressure’ may be a euphemism seem clear that Big Pharma has decided to harvest its invest-
for death”; and it does not refer to existing evidence of the con-
ments in development. At least some of the considerable na-
siderable risks that may exist for some potential users and the tional expenditures on drugs each year is due to inappropriate
number of deaths that have been associated with the inappro-
prescribing for conditions that do not require drugs – the dis-
priate use of Viagra. In 1998 Brooks showed evidence that 69 ease mongering spoken of earlier. Another considerable element
deaths associated with the inappropriate use of Viagra with le-
of the expenditure is related to prescribing newer more expen-
gitimately prescribed but contra-indicated drugs. HSNZ make sive medications where older less expensive medications would
reference to a number of studies that show that there are many be just as good. This would seem to be borne out by Stern and
contra-indications for Viagra, and they feel that these contra-in-
Ehrenberg’s (2003) finding that 80% of pharmaceutical market-
dications should be more openly and clearly flagged. For similar ing managers believed that the easiest way to increase the sales
issues see also Blondeel (1997), www.bbc.co.uk/panorama - Se-
of their drugs was to get existing users to prescribe them more.
They argue however that pharmaceutical firms would be bet-
ter advised to acquire more customers, i.e. generate more occa-
sions for prescribing. Either way the implications for costs are
Disease Mongering
enormous. It is important to note though that that increased
prescribing is only cost inefficient if medications are prescribed
Thomas (1980) wrote of his concerns about the potentially inappropriately. If they are being used appropriately they may
negative impacts of increased drug and disease promotion. He save money from other more expensive elements of the health
felt that the constant emphasis on health risk and the promul-
care system, in particular hospital costs.
gation of the view that people are “fundamentally fragile, always
on the verge of mortal disease” was simply untrue. He sug-
gested that “The new danger to our well-being, if we continue What needs to happen?
to listen to all the talk, is in becoming a nation of healthy hy-
pochondriacs, living gingerly, worrying ourselves half to death.”
Current regulation of marketing practice by pharmaceutical
This view is also held by Mintzes (2002) who gives examples manufacturing consortia such as the Association of the British
of the direct relationship between exposure to advertising and Pharmaceutical Industry (ABPI), US PhRMA organisation
enrolment in drug regimens that are not always necessary or ap-
and the Irish Pharmaceutical Healthcare Association (IPHA)
propriate. Shapiro and Shultz (2001) argue that the increased is more than forgiving. For example in the case of sponsorship
public exposure to media advertising and discussion of antide-
of sponsorship of overseas travel the IPHA has the following
pressants such as Paxil (Seroxat) and Prozac have directly led to to say:
the inappropriate prescribing of these drugs to patients whose
“Companies may be requested to sponsor the travel expens-
symptoms do not merit such extreme therapies, a view shared es of a member of the health professions attending and overseas
EJBO Electronic Journal of Business Ethics and Organization Studies
international scientific conference. The expenses incurred by the
delegate in attending such a conference can reasonably be paid A way forward
to the delegate by the company and this is acceptable. Hospital-
ity extended by a company to a delegate attending an overseas
Clearly there are many aspects to this issue, not least the ar-
meeting must be reasonable in level and secondary to the major gument frequently put forward by Big Pharma that they fund
purpose of the occasion at which it is provided. Hospitality must the majority of research into often life-saving therapies and are
not be extended beyond health professionals.” (IPHA 1999)
therefore net contributors to society. There are also obviously
Similarly the ABPI has this to say about members’ involve-
the wider philosophical debates about the degree to which soci-
ment in continuing medical education: “the pharmaceutical in-
eties should be regulated, and issues around defining reasonable
dustry is also deeply involved in doctors’ continuing education, profit and appropriate business behaviour which beleagur many
and helps in training prescribers in the uses and techniques of sectors, not just Big Pharma. However not withstanding these
new medicines. G.P.s and other health professionals would find elements, I argue that two things should happen –
it difficult to keep up to date with scientific and medical ad-
Independent monitoring bodies should be established
vances without these initiatives.” (ABPI 2003)They go further to police marketing codes of practice with real penalties and,
in a position paper to say that the ABPI directly complies with
increased attention should be paid to the education of
UK statutory regulations on the marketing and promotion of the consumers of pharmaceutical advertising, in particular those
The US equivalent organization PhRMA adopted a volun-
tary code of practice for its member organizations in July 2002
that seems to propose the toning down of the extremes of gift-
Independent monitoring of marketing codes of
giving and inducements to doctors. However in reading the practice with real penalties
question and answer section ay the end of the code of practice it
is clear this is not the case. Gift giving and generous hospitality,
The pharmaceutical industry should not be self-regulating
and in some cases, fees for endorsement of products, are still in this vital area since misleading/inaccurate pharmaceutical
very much allowable. It is important to note that in the United promotion can have very serious impacts. Rather governments
States while PhRMA has its own voluntary code, the FDA still and national medicines agencies should take pro-active stances
actively monitors promotion, though it lacks the resources to in monitoring drug advertising and promotion practices, with
monitor more than a fraction of all promotion, and there are real penalties, in particular substantial fines. The current reac-
tive and non-dedicated status of monitoring agencies is inad-
This begs the question is it appropriate to allow an industry equate. This is in part due to the inadequate resourcing of such
such as Big Pharma to self-regulate in the area of marketing? organisations. This might be countered by an arrangement such
Should this not be the role of government, or wider industry as that underpinning the Superfund of the US Environmental
organs such as the International Chamber of Commerce (ICC). Protection Agency, where industry members pay a levy to fund
Taking the ICC role first it is clear that while individual phar-
the monitoring of environmental impact and the policing of
maceutical companies may well be members of the ICC, they polluting behaviour. Similarly, in 2002, the U.S. Government’s
do not often adhere to the again voluntary code of marketing Sarbanes-Oxley Act established the Public Company Account-
practice which states the following about sales promotion for ing Oversight Board to be funded by industry contribution,
example “all sales promotions should be legal, decent and honest which replaced industry self-regulation, which was seen to have
… all sales promotions should be so designed and conducted as failed following the major financial scandals associated with En-
to avoid causing justifiable disappointment or giving any other ron and WorldCom.
grounds for reasonable complaint” (ICC2002). Would phar-
In addition to adequately funded monitoring bodies to over-
maceutical promotion meet these standards? The evidence of see marketing practice, the system of penalties for infringement
research into the promotion of products such as Viagra , Serox-
need to be overhauled. While many countries have codes of
at/Paxil and Baycol would suggest not. The fundamental issue practice, and agreed understandings as to appropriate practice,
in the case of industry organization codes (including ICC) is such as the U.S. FDA code of practice, often the penalty sys-
the real absence of sanction. PhRMA’s code of practice is vol-
tems are inadequate to the point of being ineffectual.
untary, as are IPHA’s and ABPI’s, and “each member company
For example under the United Kingdom’s ABPI code of
is strongly encouraged to adopt procedures to ensure adherence marketing practice complaints about infringement can be made
to this code”(PhRMA 2002). It could be argued that such vol-
by anyone including members of the public. The company has
untary self-regulatory codes are not designed to ensure accu-
six weeks to respond in writing, with a defense of the issue at
racy and objectivity, but are instead set up to ‘level the playing hand. This complaint is then considered by a panel of three peo-
field’ among member companies. An examination of the origin ple with legal backgrounds, on behalf of the ABPI. If the com-
of complaints to such bodies indicates that most tend to come pany is found to be in breach of the code of practice they will
from other drug companies (Lexchin 2003).
incur a fine in the order of £1000 (approx US$1670) and be
required to give an undertaking to withdraw all offending ma-
terials within approximately two weeks. If the breach is judged
Role of Government
to be serious, and to “bring the industry into disrepute” then the
fine will be more severe, but still relatively small.
While there are government agencies charged with monitor-
If one considers the profits to be made within the pharma-
ing the marketing of medicines, typically this is one of many ceutical sector, and the potential human risks associated with
briefs for these agencies and is often only in a reactive fashion. misleading or inaccurate promotion, it would seem clear that
In other words such monitoring as does occur, occurs only in the penalties for breaches of marketing codes of practice should
response to complaints, and even then is often very slow and be commensurate. It could well be argued that the fines that
apply in many countries are financially insignificant to Big Phar-
EJBO Electronic Journal of Business Ethics and Organization Studies
ma, and therefore considered effectively a cost of doing business schools, for example, across Ireland and Britain shows that at
present there is no education in the area of business and in par-
ticular marketing (English Maher 2003). This should surely be
addressed, so that at least doctors, and others with prescrib-
Increased education of consumers and those with
ing powers, would understand the techniques and practices to
prescribing powers
which they will be subjected as practitioners.
Initiatives are being taken to increase awareness of the na-
In addition to increasing the monitoring and policing of ture and impacts of pharmaceutical promotion in the United
Big Pharma promotion, it would seem prudent to increase the States. Significantly the American Medical Student Associa-
awareness and sophistication of the key promotion targets, tion has recently begun a campaign to regulate the relationship
through increased education about marketing. General con-
between Big Pharma and medical students (Moynihan 2003).
sumer education is difficult to achieve, as is daily evidenced by The PharmFree pledge that the American Medical Student As-
the limited success of public health promotion campaigns such sociation propose students sign includes the following “I will
as those around the health risks of smoking. That is not to sug-
make medical decisions … free from the influence of advertising
gest that it should not be attempted, but it would be unwise to or promotion. I will not accept money, gifts or hospitality that
expect it to have immediate and universal impacts. While gener-
will create a conflict of interest in my education, practice, teach-
al consumer awareness may be difficult to achieve, considerable ing or research.” The tenor of the PharmFree pledge should be
opportunity exists for increasing the knowledge base of those the guiding point for setting standards of practice for pharma-
with prescribing powers. A review of the curricula of medical ceutical marketing.
Bibliography
ABPI (2003) “Code of Practice for the Pharmaceutical Industry 2003”
in Japan: Background and the experience of US firms” European
Association of the British Pharmaceutical Industry: London
Aitken, M., Holt, F. (2000) “A prescription for direct drug marketing”
EFPIA (2002) The Pharmaceutical Industry in Figures 2002 edition
European Federation of Pharmaceutical Industries and Associations:
Banks, JW, Mainour, AG (1992) “Attitudes of medical school faculty
towards gifts from the pharmaceutical industry” Acad Med 67: 610-
English-Maher, M. (2003) “The Role of the Clinician in Service
Delivery” unpublished M.Sc research work
Barnes, M.L. (2003) “Marketing to a segment of one” Pharmaceutical
Essif, M. (2001) “Prescription drugs are crossing borders to buyers”
www.bbc.co.uk (2000)- “G.P.s seize on Prozac to treat PMS” 29 Sep
Ess, S.M., Schneeweiss, S., Szucs, T.D. (2003) “European Healthcare
Policies for Control ing Drug Expenditure” Pharmacoeconomics
Blondeel, L. (1997) “Advertisement for nifedipine does not mention
admitted shortcomings of study” British Medical Journal 315: 1621
Farrell, L. (2000) “O Liberty! What crimes are committed in thy name!”
Bloom, B.S. (1999) Annals of Internal Medicine Dec 7
Boseley, S. (1999) “Drug firm asks public to insist NHS buys its product”
Flynn, L.T. (1999) “Does direct to consumer advertising of prescription
drugs benefit the public’s health? – Yes” in American Council on
Brooks, A. (1998) “Viagra is licensed in Europe but rationed in Britain”
Gopal, K. (2002) “GSK face bribe charges, changing of the guard”
Burton, B. (2003) “Ban Direct to Consumer Advertising , Report
Recommends” British Medical Journal 326:467
Gottlieb, S. (2002) “Congress criticizes drugs industry for misleading
Burton, B., Rowell, A. (2003) “Unhealthy spin” British Medical Journal
advertising” British Medical Journal 325:137
Hayes, T.M., Al ery, L.A., Harding, K.G., Owen, P.A. (1990)
Calfee, J. (2002) “Public Policy Issues in Direct-to-Consumer Advertising
“Continuing education for general practice and the role of the
of Prescription Drugs” Journal of Public Policy and Marketing 21 (2)
pharmaceutical industry” British Journal of General Practice 40
Canadian Medical Association Journal (2003) Sep 30, 169 (7)
Healthy Skepticism New Zealand (2000) “Does direct to consumer
Chren, MM, Landefeld CS, Murray TH (1989) “Doctors, drug
promotion of Viagra risk lives?” Healthy Skepticism New Zealand 3
companies and gifts” Journal of the Australian Medical Association
Herxheimer, A. (2003) “Relationships between the pharmaceutical
Chren, MM, Landefeld S (1994) “Physicians’ behaviour and their
industry and patient organisations” British Medical Journal 326:
interactions with drug companies” Journal of the Australian Medical
Horrobin, D.F. (2000) “Innovation in the pharmaceutical industry”
Corstjens, M. (1991) Marketing Strategy in the Pharmaceutical Industry
Journal of the Royal Society of Medicine Jul 93, 341-345
ICC (2002) “International Code of Practice of Sales Promotion”
Davidoff, F., DeAngelis C.D., Drazen, J.M., Hoey, J., Hojgaard,
International Chamber of Commerce www.iccwbo.org
L., Horton, R. et al (2001) “Sponsorship, Authorship and
IPHA (1999) “Code of Marketing Practice for the Pharmaceutical
Industry” Irish Pharmaceutical Healthcare Association: Dublin
De Mortanges, C.P., Rietbrock, JW (1997) “Marketing pharmaceuticals
Jeffries, M. (2000) “The Mark of Zorro” Pharmaceutical Marketing May
EJBO Electronic Journal of Business Ethics and Organization Studies
Komesaroff, P.A., Kerridge, I.H. (2002) “Ethical issues concerning the
Oldham, J. (2003) “Mood drug attacker avoids jail” The Scotsman Jun 19
relationships between medical practitioners and the pharmaceutical
PhRMA (2002) “PhRMA code on interactions with healthcare
industry” The Medical Journal of Australia 2 Feb 176 3:118-121
professionals” in www.phrma.org/publications/policy/2002-04-
Lerer, L. (2002) “Pharmaceutical marketing segmentation in the age of
the Internet” International Journal of Medicine Marketing 2,2 159-
Peay, M.Y., Peay, E.R. (1988) “The role of commercial sources in the
adoption of a new drug” Soc Sci Med 26: 1183-1189
Lexchin, J., Mintzes, B. (2002) “Direct-to-consumer advertising of
Prawirosujanto, S. (2001) “Doctors Prescriptions” Jakarta Post 29th June
prescription drugs: the evidence says no” Journal of Public Policy and
Quality and Safety in Healthcare April 2003
Maguire, P. (1999) “How direct to consumer advertising is putting the
Revill, J. (2003) “Female sex illness: is it in the head or in the genes?” The
squeeze on physicians” American Col ege of Physicians – American
Society of Internal Medicine Observer March
Riccardi, F. (2002) “Healthcare Providers and Pharmaceutical
McInney WP, Schiedermeyer DL, Lurie N et al (1990) Attitudes
Companies: Is there a prescription for Ethical Relationships?” Journal
of internal medicine faculty and residents towards professional
interaction with pharmaceutical sales representatives” Journal of the
Robinson, J. (2001) “Prescription Games” Simon and Schulster:London
Australian Medical Association 264: 1693-1697
Shapiro, J.P., Shultz, S. (2001) “Prescriptions: How your doctor makes
Medawar, C. (1997) “The Antidepressant Web – marketing depression
the choice” U.S. News and World Report 130:7 58 - 62
and making medicines work” International Journal of Risk and Safety
Smith, R. (2003) “Medical journals and pharmaceutical companies:
uneasy bedfel ows” British Medical Journal 326: 1202-1205
Medawar, C. (2002) “Promotion of prescription drugs: trade tactics?”
Stern, P., Ehrenberg, A. (2003) “Expectations vs. Reality” Marketing
Medical Marketing and Media (2003) “Court Documents Show Merck
Strout, E. (2001) “Doctoring Sales” Sales and Marketing Management
Medco received $3 billion in pharma rebates” editorial Medical
Thomas, L. (1980) “The Medusa and the Snail” New York: Bantam
Mintzes, B. (2002) “Direct to consumer advertising is medicalising
normal human experience” British Medical Journal 324: 908-911
Thomson, A.N., Craig, B.J., Barnham, P.M. (1994) “Attitudes of general
Mintzes, B., Barer, M.L., Kravitz, R.L., Kazanjian, A., Bassett, K.,
practitioners in New Zealand to pharmaceutical representatives”
Lexchin, J., Evans, R.G., Pan, R., Marion, S.A. (2002) “Influence of
British Journal of General Practice 44 220-223
direct to consumer pharmaceutical advertising and patients’ requests
Turone, F. (2003) “Italian police investigate GSK Italy for bribery” British
on prescribing decisions: two site cross sectional survey” British
Wazana, A. (2000) “Physicians and the pharmaceutical industry. Is a gift
Moynihan, R. (2003) “Who pays for the pizza? Redefining the
ever just a gift?” Journal of the Australian Medical Association 283:
relationships between doctors and drug companies. 1: Entanglement”
Moynihan, R. (2003) “Who pays for the pizza? Redefining
the relationships between doctors and drug companies. 2: Disentanglement” British Medical Journal 326: 1193-1196
Joan BuckleyDept. of Management and MarketingUniversity College CorkCorkIrelandEmail: jb@ucc.ieTel: +353 21 4902928Fax: +353 21 4903377
Joan Buckley is a lecturer in the Department of Management and Marketing at University College Cork, Ireland.
Augustana College Note: This is a Summary of Benefits; please refer to the Plan Document for a full description of benefits, limitations and maximums. Medical Expense Benefits Limitations and Maximums In-Network Out-of-Network Annual Deductible: Annual Out-of-Pocket Maximum: (includes Co-Insurance) Does not include Deductible, Drug Co-Pays, penalties for failure to pre-cer
 EJBO Electronic Journal of Business Ethics and Organization Studies
from analgesics such as paracetamol to anti-histamines. What broadcast DTCA of these drugs has resulted in increased “pull”
is categorized as OTC varies from country to country and is de-
from consumers. In both the United States and New Zealand
pendent on the local legislative framework – usually a national DTCA of prescription drugs occurs with considerable effect, as
medicines authority, so for example in the United States some will be discussed below. A further source of ‘indirect’ pull has
been the impact of the Internet on pharmaceutical promotion,
Corstjens (1991) identifies four main buying parties for pre-
1. Prescriber – prescribing rights vary internationally and
this category may include doctors, dentists, pharmacists, nurses Direct to consumer promotion –
EJBO Electronic Journal of Business Ethics and Organization Studies
from analgesics such as paracetamol to anti-histamines. What broadcast DTCA of these drugs has resulted in increased “pull”
is categorized as OTC varies from country to country and is de-
from consumers. In both the United States and New Zealand
pendent on the local legislative framework – usually a national DTCA of prescription drugs occurs with considerable effect, as
medicines authority, so for example in the United States some will be discussed below. A further source of ‘indirect’ pull has
been the impact of the Internet on pharmaceutical promotion,
Corstjens (1991) identifies four main buying parties for pre-
1. Prescriber – prescribing rights vary internationally and
this category may include doctors, dentists, pharmacists, nurses Direct to consumer promotion –