Tadalafil entfaltet seine Wirkung über eine selektive Hemmung der PDE5, wodurch die Konzentration von cGMP im glatten Muskelgewebe stabil bleibt. Diese biochemische Modulation resultiert in einer langanhaltenden Relaxation der Gefäßwände. Der Wirkstoff wird nach oraler Einnahme effizient resorbiert, mit einer Bioverfügbarkeit von rund 80 %. Seine Halbwertszeit von bis zu 36 Stunden ist innerhalb dieser Substanzklasse außergewöhnlich. Abgebaut wird er in der Leber, hauptsächlich durch CYP3A4, mit anschließender biliärer Exkretion. Typische unerwünschte Wirkungen entstehen durch eine verstärkte Vasodilatation, etwa Kopfschmerzen oder Flush. Pharmakologisch wird cialis generika vor allem durch die verlängerte Wirkungsdauer charakterisiert.
Forensischinstituut.nl
Psychopharmacology (2007) 191:951–959DOI 10.1007/s00213-006-0669-8
Cognitive, psychomotor and actual driving performancein healthy volunteers after immediate and extended releaseformulations of alprazolam 1 mg
Tim R. M. Leufkens & Annemiek Vermeeren &Beitske E. Smink & Peter van Ruitenbeek &Johannes G. Ramaekers
Received: 8 August 2006 / Accepted: 6 December 2006 / Published online: 12 January 2007
magnitude of impairment in the driving test observed with
Rationale Alprazolam extended-release (XR) is approved
alprazolam XR was about half that observed with alprazo-
for the treatment of panic disorder. This sustained formu-
lam IR. Laboratory test results were in line with the driving
lation is absorbed in a delayed manner and is therefore
expected to produce fewer and less severe side effects than
Conclusions The acute impairing effects of alprazolam XR
its immediate release equivalent (alprazolam IR). The effect
1 mg on driving and psychomotor functions were generally
of alprazolam XR on potentially dangerous daily activities,
less, as compared to its immediate-release equivalent, but
such as driving a car, is expected to be less as compared to
still of sufficient magnitude to increase the risk of
becoming involved in traffic accidents.
Objectives The present study was designed to compare theeffects of alprazolam XR (1 mg) and alprazolam IR (1 mg)
Keywords Alprazolam XR . Driving . Cognition .
on actual driving ability and cognitive function.
Psychomotor performance . Serum concentration .
Method Eighteen healthy volunteers (aged 20–45 years)
participated in a double-blind, placebo-controlled, three-way crossover study. At 4 h post-dose, subjects performed astandardized driving test on a primary highway in normaltraffic. Cognitive and psychomotor tests were assessed 1,2.5, and 5.5 h post-dose. Memory functioning was
measured only 1 h after administration. Results Both formulations severely impaired driving per-
Daytime sedation and impairment of psychomotor and
formance between 4 and 5 h after administration. The
cognitive functioning is one of the main problems associ-ated with the use of benzodiazepine anxiolytics. This poses
T. R. M. Leufkens A. Vermeeren P. van Ruitenbeek
a crucial problem for users of these drugs who must operate
vehicles. Epidemiological studies have shown that use of
Experimental Psychopharmacology Unit, Brain and Behavior
benzodiazepines is associated with an increased risk of car
Institute, Faculty of Psychology, Maastricht University,
Experimental studies have shown, however, that effects on
driving performance vary depending on the drug, dose, and
The Netherlands Forensic Institute (NFI),
Alprazolam is the most frequently used benzodiazepine
in the treatment of panic disorder and anxiety (Isbister et al.
; Moroz RxList ; Verster et al. ). It is a
Department of Neurocognition, Faculty of Psychology,
1,4 triazolobenzodiazepine and available in two formula-
tions, an immediate release (IR) formulation and an
P.O. Box 616, 6200 MD Maastricht, The Netherlandse-mail: t.leufkens@psychology.unimaas.nl
extended release (XR) formulation. Alprazolam IR is
rapidly absorbed and has a relatively short elimination half-
of studies (reviews: Ramaekers ; Vermeeren
life ranging between 10 and 18 h (Greenblatt and Wright
Recently, it was applied in a study to assess the effect of a
; Moroz ). After oral administration of alprazolam
single dose of alprazolam IR 1 mg and placebo on actual
IR 1 mg, peak plasma concentrations ranging from 12 to
driving performance in 20 healthy young volunteers
22 μg/l are reached within 0.7 to 1.8 h after intake
(Verster et al. ). That study showed that alprazolam
(Greenblatt and Wright ). Alprazolam IR is mainly
IR produced severe impairment of road tracking control
prescribed in units of 0.25, 0.50, or 1.00 mg three times
equivalent to the effect produced by a blood alcohol
daily for patients suffering from anxiety, but daily doses can
be raised to 10 mg for patients suffering from panic
The primary purpose of the current study was to
compare the effects of alprazolam XR with those of
Patients using alprazolam IR report benzodiazepine-
alprazolam IR on performance of healthy subjects in a
related adverse events, such as drowsiness, dizziness, and
standardized highway driving test. It was expected that
reduced alertness (Verster and Volkerts A vast
driving impairment would be less after alprazolam XR as
amount of studies have shown that alprazolam IR in doses
compared with alprazolam IR, due to differences in the
of 0.5 mg and higher impairs a variety of cognitive and
pharmacokinetic profiles of both formulations. The second-
psychomotor skills such as memory, speed of responses,
ary purpose was to compare the effects on cognitive and
and tracking performance (Bertz et al. ; Ellinwood et
psychomotor functioning related to driving in a controlled
Scavone et al. ; Smith et al. Subhan et al. Vermeeren et al. ; Verster et al.
Alprazolam XR was developed to reduce the adverse
events associated with alprazolam IR. It produces peakplasma concentrations that are about 50% of a similar dose
of the IR formulation and occur between 5 and 12 h afteradministration (Busto et al. ; Eller and Della-Coletta
Eighteen healthy volunteers (nine men and nine women)
; Fleishaker et al. ; Glue et al. Alprazolam
were recruited by means of advertisements in local news-
XR produced fewer and less severe side effects than its IR
papers and public buildings. Their mean ±SE age was 32.3±
equivalent. Moreover, it has been shown that cognitive and
2.0 years. Volunteers were screened by a telephone inter-
psychomotor performance is less impaired after alprazolam
view, health questionnaire, and medical examination. The
XR than after alprazolam IR (Busto et al. Mumford et
medical examination included blood hematology and chem-
istry, urinalysis, drug and pregnancy screening, and a 12-lead
It is unclear, however, if a reduction in performance
electrocardiogram. Inclusion criteria were age between 21
impairment observed in laboratory tests of psychomotor
and 45 years, good physical and mental health, body mass
function and cognition after alprazolam XR will have any
index between 18 and 28 kg/m2, possession of a driving
implications for drivers who are being treated with
license for more than 3 years, and average driving
alprazolam. In general, the validity of short psychomotor
experience of at least 5000 km/year. Volunteers with any
tests for predicting actual driving performance is limited. At
cardiovascular, endocrine, psychiatric, and/or neurological
best, drug-induced impairments in psychomotor tests are
condition were excluded, as were subjects with a history of
only moderately correlated to drug-induced impairment in
drug abuse or currently using psychoactive medication,
driving performance as assessed in on-the-road driving
hypotension (<90/50 mmHg), liver disorder, pregnancy or
tests. Consequently, it is widely accepted in the drug and
lactation, and drinking more than 20 alcoholic consump-
driving community that experimental studies for establish-
ing the driving hazard of a medicinal drug should proceed
From 1 week before participation in the study until
from conventional psychomotor tests to driving simulators
completion of the last treatment period, subjects were not
and actual driving tests. Therefore, the final conclusions
allowed to use any prescribed medicines or drugs of abuse.
concerning a drug’s impairing effect on driving should be
During the study period, it was not allowed to participate in
based on combined results from these studies (ICADTS
any other biomedical research. Subjects had to refrain from
alcohol and caffeine 24 h before testing. On test days,
The present study was designed to establish the effects
subjects were not allowed to consume any food 3 h before
of alprazolam XR on actual driving performance as
arrival. During testing, smoking was prohibited.
assessed in a standard on-the-road driving test (O’Hanlon
The study’s approval was obtained from the medical
). This test has been used repeatedly for assessing
ethics committee of Maastricht University. The study was
medicinal drug effects on actual driving in a large number
conducted according to the code of ethics on human
experimentation established by the World Medical Associ-
a visual search task in which the subject has to monitor 24
ation’s Declaration of Helsinki (1964) and amended in
asynchronously changing single digits presented in the four
Edinburgh (2000). After complete description of the study
corners of a screen. The subjects are instructed to remove
to the subjects, written informed consent was obtained.
their foot from a pedal as rapidly as possible whenever theydetect the digit ‘2’. The main performance parameters are
average tracking error (in mm) and number of controllosses in the tracking task and number of misses and speed
The study was conducted according to a double-blind,
of target detection (in ms) in the visual search task. These
placebo-controlled, three-way crossover design. Treatments
parameters are transformed to standard (z) scores for each
were single oral doses of alprazolam 1 mg IR, alprazolam
task. Performance in this test has proven sensitive to the
1 mg XR, and placebo. Study medication was supplied in
effects of many sedative drugs such as doses of alcohol,
three capsules (double dummy) at 9 A.M. of each test day.
antidepressants, antipsychotics, antihistamines, and the
Treatment orders were balanced by randomly assigning six
residual effects of hypnotics (Ramaekers et al. ; Robbe
treatment orders to 18 subjects. The minimum period
and O’Hanlon Vermeeren et al. ; Vuurman et al.
between successive treatments was 7 days.
The Stop Signal Task assesses inhibitory control, defined
as the ability to stop a pending thought or action (Logan). The paradigm consists of two concurrent tasks, i.e.,
Before the first treatment period, all subjects received a
a stop and a go task. The current test was adapted from an
comprehensive training of the driving and laboratory tasks.
earlier version by Fillmore et al. (and has been
The standardized highway driving test was undertaken
validated for showing stimulant and sedative drug effects
between 4 and 5 h after dosing, i.e., the time plasma
(Ramaekers and Kuypers ). The go signals are four
concentrations of the XR formulation were expected to be
letters (A, B, C, or D) presented one at a time in the center
at a maximum. The Stop Signal Task and a Divided
of a computer screen. Subjects are required to respond to
Attention Task were performed at 1, 2.5, and 5.5 h after
each letter as quickly as possible by pressing one of two
dosing. A Word Learning Task was performed at 1 h post-
response buttons by either the left (A or C) or right (B or D)
dose. Subjects consumed two standardized light meals 0.5 h
index finger. In the stop task, subjects are required to
withhold any response in case a stop signal (a visual cueappearing in one of the four corners of the screen) is
presented. Stop signals are presented 12 times at each of thefour delays after the onset of a letter: 50, 150, 250, 350 ms
In the 1-h driving test (O’Hanlon subjects operate a
The dependent variables are reaction times to go signals
specially instrumented vehicle over a 100-km (61-mi)
(Go RT), the average delay needed to inhibit successfully
primary highway circuit while maintaining a constant speed
the ongoing response (stop signal reaction time, SSRT) and
of 95 km/h (58 mi/h) and a steady lateral position between
the delineated boundaries of the right (slower) traffic lane.
The Word Learning Task assesses memory for verbal
Subjects are accompanied by a licensed driving instructor
information (Rey In this test, 15 monosyllabic nouns
with access to dual controls. During the test, the car’s speed
are sequentially presented on a computer screen for 2 s, and
and lateral position with respect to left lane-line are
the subject is required to read the words aloud. At the end
continuously recorded. These signals are edited off-line to
of the sequence, the subject is asked to recall as many
yield the Standard Deviation of Lateral Position (SDLP in
words as possible in any order. This procedure is repeated
centimeters) which is taken as the primary outcome
five times, and the total number of correct recalls in five
variable. SDLP is a measure of road tracking error or
trials is referred to as the Immediate Recall Score (IRS).
‘weaving’. SDLP has proven to be sensitive to the sedative
After a delay of at least 20 min, the subject is again
and stimulating effects of various psychoactive drugs such
required to recall as many words as possible. During this
as anxiolytics (O’Hanlon et al. Verster et al. ),
trial, the nouns are not presented. The total number of
hypnotics (Vermeeren antidepressants (Ramaekers
correct recalls is referred to as the Delayed Recall Score
), and antihistamines (O’Hanlon and Ramaekers
(DRS). Finally, a sequence of 30 monosyllabic nouns is
presented, containing 15 nouns from the original set and 15
The Divided Attention Task measures the ability to per-
new nouns in random order. The subject has to indicate
form two tasks simultaneously during 12 min (Moskowitz
whether a noun originates from the old or from the new set.
). The primary subtask is a compensatory tracking task
The total number of correct indications is referred to as the
set at a constant level of difficulty. The secondary subtask is
Recognition Score (RS). The reaction time of decision is
measured and is referred to as the Recognition Reaction
forensic case work, calibration curves are included in each
Time (RRT). Performance in this test has previously been
shown to be sensitive to the effects of alprazolam IR indoses of 0.5 and 1 mg (Vermeeren et al.
Sample size was based on a power calculation for detectinga clinically relevant effect of 2.4 cm in the primary measure
Alprazolam was determined by measuring serum concen-
of this study, the SDLP. This change corresponds to the
trations. Blood samples were collected at 55 min and 6 h
effects of alcohol on SDLP, whereas BACs are 0.5 g/l as
after ingestion of the drug. Samples were centrifuged after a
measured in a previous study (Louwerens et al.
clotting period, and serum was frozen at −20°C until
Given that test–retest reliability of the driving test is at least
analyses for pharmacokinetic assessments. Serum was
r=0.70, a group of 18 subjects should permit detection of a
analyzed for serum concentrations of alprazolam and its
mean change in SDLP of 2.0 cm, with a power of at least
metabolite α-hydroxy-alprazolam using a Liquid Chroma-
tography-Tandem Mass Spectometry Method (LC-MS-MS)
The global model used in the analysis of variance
(ANOVA) of all cognitive and psychomotor parameters
Internal standards, d5-alprazolam and d5-α-hydroxy-
included subject, period, treatment, and time of testing. In
alprazolam, were added to 1.0 ml serum sample before
case of a significant overall effect of treatment, a
solid-phase extraction (Oasis HLB®, Waters, Etten-Leur,
subsequent analysis for comparing separate drug treatments
The Netherlands). The analytes were eluted from the
was conducted using three simple contrasts.
cartridges with 1.5 ml acetonitrile after washing with 2 ml
All statistical analyses were done by using the Statistical
water and 2 ml acetonitrile/water 10% v/v. The serum
Package for the Social Sciences (SPSS) statistical program
extracts were evaporated and reconstituted in 50 μl aceto-
(version 12.0.1 for Windows; SPSS, Chicago, IL).
nitrile/water 20% v/v before analysis.
The LC-MS system consisted of a TSP Spectra System
(Finnigan, Breda, The Netherlands), including an SN4000
controller, a vacuum degasser (SCM 1000), a pump(P4000), and an auto sampler (AS3000), connected to an
A summary of the cognitive, driving, and psychomotor
ion trap mass spectrometer (LCQ, Finnigan). Chromato-
graphic data were acquired and processed using X-calibur™ 1.2 software (Finnigan). The method used an
Atlantis C18 column (150×2.1 mm, Waters, Etten-Leur,The Netherlands). Injection volume was 10 μl. The gradient
Word Recognition Test data were incomplete for five
used in this LC-MS (MS) method was acetonitrile/formic
subjects and Stop Signal Task data were incomplete for
acid (0.005 M), 10% to 90% v/v acetonitrile. The time
six subjects due to technical problems. Only complete data
course of the gradient was as follows: t=0–1 min (10–40%
v/v acetonitrile), t=1–7 min (40 v/v % acetonitrile), t=7–8 min (40–90% v/v acetonitrile), t=8–9 min (90% v/v
acetonitrile), t=9–10 min (90–10% v/v acetonitrile). Parentions (m/z 309, 314, 325, and 330 for alprazolam, d5-
Ten driving tests (18.5% out of 54 comprising the complete
alprazolam, α-hydroxy-alprazolam, and d5-α-hydroxy-
data set) were terminated prematurely because the driving
alprazolam, respectively) and product ions (m/z 274 and
instructors judged the subject to be too drowsy to continue
281 for alprazolam, m/z 279 and 286 for d5-alprazolam,
safely. They terminated seven rides (38.9% out of 18
m/z 279, 297, and 307 for α-hydroxy-alprazolam, and m/z
comprising one condition) in the IR condition and three
284, 302, and 312 for d5-α-hydroxy-alprazolam) were
rides (16.7%) in the XR condition. The SDLP scores were
calculated from the data collected until termination of each
The linear range for the assay was 1–10 ng/ml for
alprazolam and 0.5–5 ng/ml for α-hydroxy-alprazolam. The
There was a significant treatment effect [F(2,16)=31.89,
limit of quantification (concentration with an intra-day
p < 0.001]. Contrast analysis revealed that both drug
standard deviation of 20%) was 1 ng/ml for alprazolam and
formulations significantly increased SDLP [IR: F(1,17)=
0.5–1 ng/ml for α-hydroxy-alprazolam. The accuracy was
67.44, p<0.001; XR: F(1,17)=36.86, p<0.001]. However,
satisfactory (deviation from calibrated external control
mean SDLP after alprazolam XR was significantly lower as
10%). Inter-day precision was not determined, because in
compared to alprazolam IR [F(1,17)=34.37, p<0.001].
Table 1 Summary of the results of the Road Tracking Test and Cognitive and Psychomotor Tests in healthy subjects in a crossover trial ofalprazolam IR (1 mg), alprazolam XR (1 mg), and placebo (n=18)
PLA Placebo, IR alprazolam Immediate Release, XR alprazolam Extended Release, NS not significant, SDLP standard deviation of lateral position,
SDS standard deviation of speed, IRS immediate recall score, DRS delayed recall score, RS recognition score, RRT recognition reaction time, FAfalse alarms, z-AE z-score of average tracking error, z-ln(cl) z-score of log transformed total number of control losses, z-RT z-score of reactiontime, z-ln(mi) z-score of log transformed total number of misses
Figure shows that SDLP increased with approximately
showed that tracking performance was significantly im-
8 cm in the IR condition and 4 cm in the XR condition as
paired at 1, 2.5, and 5.5 h after administration of alprazolam
IR 1 mg [1 h: F(1,17)=15.88, p<0.001; 2.5 h: F(1,17)=
No overall differences between placebo and drug were
15.14, p < 0.001; 5.5 h: F(1,17) = 12.40, p < 0.01] and
found on mean speed and speed variability.
alprazolam XR 1 mg [1 h: F(1,17) =6.31, p<0.05; 2.5 h F(1,17) =7.00, p<0.05; 5.5 h: F(1,17) =12.26, p<0.01]. The
effects of the XR formulation were less severe, however, thanthose of the IR formulation at 1 h [F(1,17)=15.42, p<0.05]
The distributions of control losses and misses were
and 2.5 h post-dose [F(1,17)=21.32, p<0.05] but no longer at
highly skewed. Therefore, they were transformed to their
natural log (ln) scores before transformation to z-scores.
A significant overall treatment effect in target detection
ANOVA of the sum score of the z-scores of the average
performance, as measured by the sum of the z-scores of the
error and natural log of the total number of control losses
reaction time and natural log of total number of misses, was
revealed a significant overall treatment effect [F(2,16)=
found [F(2,16) =5.72, p<0.05]. Analyses at separate times
11.74, p<0.001]. Effects of treatments were further ana-
after administration revealed a significant impairment on
lyzed at separate times after drug intake. These analyses
target detection by alprazolam IR compared to placebo at
Fig. 1 Mean (±SE) StandardDeviation of Lateral Position(SDLP) in each drug condition. a is significantly different fromplacebo (p<0.001) and b issignificantly different fromalprazolam XR (p<0.001)
all times of measurement [F(1,17) =6.89, p<0.05]. Alpra-
after ingestion [F(1,11)=109.92, p<0.001; F(1,11)=6.44,
zolam XR did not differ significantly from placebo 1 h
p<0.05, respectively] but no longer at 5.5 h post-dose.
post-dose. On 2.5 and 5.5 h post-dose, target detection
For the total number of false alarms data, analyses
differed significantly between placebo and alprazolam XR
[respectively, F(1,17)=4.46, p<0.05; F(1,17)=6.49, p<0.05]. Comparisons between both treatment conditions
revealed significant differences at 1 h and 2.5 h post-dose[respectively, F(1,17)=5.84, p<0.05; F(1,17)=6.72, p<
Analysis of the total number of words correctly recalled
0.05]. At 5.5 h after ingestion, target detection was not
over five memory trials, as reflected by the IRS, showed a
significantly different between both treatment conditions.
significant overall treatment effect [F(2,16)=9.08, p<0.01]. Placebo-drug comparisons revealed a significant impairing
effect of alprazolam IR at 1 h after administration but not ofalprazolam XR. No significant difference was found
Analysis revealed a significant overall treatment effect on
between alprazolam IR and alprazolam XR.
the go reaction time [F(2,10) =6.20, p<0.05]. Separate
The DRS also revealed a significant overall treatment
analyses for each time of testing revealed significant
effect, as delayed recall under the alprazolam IR condition
differences between treatments at 2.5 h post-dose. At that
was significantly lower than under the placebo condition [F
time, relative to placebo, the go reaction time was
(1,17) =10.22, p<0.01]. Delayed recall after alprazolam XR
significantly longer after alprazolam IR [F(1,11)=22.87, p
ingestion did not significantly differ from placebo. The
< 0.001] but not after alprazolam XR. Moreover, the
difference between alprazolam IR and alprazolam XR was
increment in reaction time after alprazolam IR was also
significant [F(1,17)=4.64, p<0.05).
significantly different from that after alprazolam XR [F
No significant effects were found on performance in the
(1,11)=23.70, p<0.001]. No interaction was found between
A significant interaction effect between treatment and
time of measurement in SSRT was found [F(2,10)=58.94,p<0.001]. Placebo drug comparisons for each time of
Mean (SE) serum concentrations for alprazolam at 55 min
testing showed that alprazolam IR increased SSRT signif-
post-dose were 4.9 (1.0) μg/l after alprazolam IR adminis-
icantly at each time of testing [F(1,11)=6.01, p<0.05],
tration and 1.7 (0.2) μg/l after alprazolam XR administra-
whereas alprazolam XR did not. SSRT after alprazolam XR
tion. After approximately 6 h of drug ingestion, mean (SE)
was significantly faster than after alprazolam IR 1 and 2.5 h
serum concentrations for alprazolam were 10.6 (0.5) μg/l
after alprazolam IR and 9.0 (0.6) μg/l after alprazolam XR.
and delayed recall in the word learning task. In contrast,
The alprazolam metabolite α-hydroxy-alprazolam was not
alprazolam XR only impaired performance in the divided
detectable in the serum. The metabolite is expected to be
attention task but not in the stop signal and memory tests,
present in plasma in unconjugated form at less than 10% of
indicating a reduction in adverse effects.
This reduction in impairing effects was most pronounced
within the first 4 h after administration of both formula-tions, when blood levels of alprazolam XR were still rising
and those of alprazolam IR were at their peak, as shown bythe serum concentrations. Within this time period, the
Results from the present study show that both alprazolam
effects of alprazolam XR were significantly less severe in
1 mg formulations administered as single doses to healthy
the majority of the tests as compared with those of
nonanxious volunteers significantly impair performance on
alprazolam IR. At 5.5 h, post-dosing performance effects
the standardized highway driving test. The IR formulation
and serum concentrations became comparable. At this point
produced a mean increase in SDLP of 8.2 cm and the XR
in time, alprazolam XR achieves peak plasma concentra-
formulation produced an increase of 3.9 cm. Although the
tions, whereas alprazolam IR plasma levels are already
magnitude of effect on SDLP was reduced by about 50%
descending. Thus, peak effects of alprazolam XR are less
after alprazolam XR, the impairment was still severe. The
acute effects of alprazolam IR and alprazolam XR would be
A potential limitation of the present study might be that
the equivalents of driving with a BAC above the legal limit
the effects were assessed only after a single dose adminis-
for alcohol in most industrialized countries, i.e., 0.5 g/l
tration of study treatments. Alprazolam-induced impairment
(Louwerens et al. BACs of above 0.5 g/l have been
may become less severe after chronic administration of
shown to progressively increase the risk of becoming
alprazolam, as it is well known that tolerance to the
involved in a serious traffic accident by a factor of 2 or
sedating effects of benzodiazepines can develop after
more (Borkenstein ). The number of driving tests that
repeated use (Curran ). However, it has also been
were prematurely terminated supported the SDLP data.
shown that tolerance to the impairing effects of benzodia-
Under the alprazolam XR condition, three (16.7%) subjects
zepines is never complete. An epidemiological study by
were not able to complete the driving test. Alprazolam IR
Neutel ) demonstrated that benzodiazepines increase
caused an early ending of the test in seven (38.9%)
the relative risk of becoming involved in traffic accidents
subjects. The most frequent reason for aborting the test
during the first week of treatment and that this risk remains,
prematurely was excessive sleepiness.
albeit to a lesser extent with passage of time. During the
The detrimental effect of alprazolam IR on driving in the
first week of treatment, the benzodiazepine users’ relative
present study is similar to that found in a previous study
risk was 13.5. After 1 month, the relative risk had declined
employing the same standardized highway driving test. In
to 2.6. The implication thus seems to be that benzodiaze-
that study, Verster et al. ) found a mean increment in
pine impairment persists over time but to a lesser degree as
SDLP of approximately 9 cm between 1–2 h after a single
observed after initial dosing. A similar pattern was found in
dose of alprazolam IR 1 mg. This indicates that sensitivity
an experimental study assessing the effects on driving
of the subjects in the present study to the effects of
performance of diazepam 5 mg treatment during 4
consecutive weeks in 12 patients with generalized anxiety
Although the laboratory tests are not expected to
disorder (Van Laar et al. Diazepam significantly
strongly predict driving performance, they usually provide
impaired driving performance as reflected by an elevated
some insight as to what extent driving is affected after drug
SDLP in the first 3 weeks of treatment. Therefore, it was
intake. Driving ability is not one distinct skill but a
concluded that driving performance of patients will be
combination of a series of mental and behavioral functions
affected at least during early, chronic treatment.
(Vermeeren and De Gier ). Therefore, performance in
It might be argued that performance of healthy subjects
laboratory tests assessing different aspects of driving can
may be different from performance of patients suffering
provide insight into what aspects of driving behavior are
from anxiety of panic disorder. Moreover, as healthy
most sensitive to the effects of a particular drug, although
volunteers do not have a history of benzodiazepine use,
performance in any single test is not highly correlated to
the effect of alprazolam may be stronger than that in
driving performance itself. As expected, alprazolam IR
patients who have already been using alprazolam for an
significantly impaired performance on all tasks as com-
extended period of time. Yet, these notions have never been
pared with placebo. It impaired tracking and peripheral
confirmed in scientific research. On the contrary, O’Hanlon
visual search in the divided attention task, response speed
et al. (have shown that driving performance after
and inhibitory control in the stop signal task, and immediate
both single and repeated doses of benzodiazepine anxio-
lytics did not differ in healthy volunteers and patients.
Greenblatt DJ, Harmatz JS, Dorsey C, Shader RI (1988) Comparative
Moreover, these authors showed that baseline and placebo
single-dose kinetics and dynamics of lorazepam, alprazolam,prazepam, and placebo. Clin Pharmacol Ther 44:326–334
performances were comparable between both groups. This
ICADTS (1999) Guidelines on experimental studies undertaken to
implies that healthy volunteer models can be used for
determine a medicinal drug’s effect on driving or skills related to
predicting drug effects on driving in patient populations.
driving. Bundes Anstalt fuer Strassenwesen (BASt), Köln
Therefore, if the effects of both formulations of alprazolam
Isbister GK, O’Regan L, Sibbritt D, Whyte IM (2004) Alprazolam is
relatively more toxic than other benzodiazepines in overdose. Br
observed in the present study also apply to anxious
individuals receiving the medications as clinical treatment,
Kroboth PD, Folan MM, Bauer KS, Tullock W, Wright CE, Sweeney
the risk of becoming involved in a car accident may be
JA (1998) Do alprazolam-induced changes in saccadic eye
movement and psychomotor function follow the same timecourse? J Clin Pharmacol 38:337–346
In conclusion, the impairing effects of alprazolam XR
Logan GD (1994) On the ability to inhibit thought and action: a users’
1 mg on driving and cognition were generally less as com-
guide to the Stop Signal Paradigm. In: Dagenbach D, Carr TH
pared to its IR equivalent but still of sufficient magnitude to
(eds) Inhibitory processes in attention, memory, and language.
increase the risk of becoming involved in traffic accidents.
Louwerens JW, Gloerich ABM, de Vries G, Brookhuis KA, O’Hanlon
JF (1987) The relationship between drivers’ blood alcohol
This research was supported by a grant from
concentration (BAC) and actual driving performance during high
speed travel. Alcohol Drugs Traffic Saf 86:183–186
We like to thank Anita van Oers, Janneke Guijaux, Roland Otten,
Moroz G (2004) High-potency benzodiazepines: recent clinical
Henk Brauers, Willy Jeurissen, Irma Brauers and Cees van Leeuwen
results. J Clin Psychiatry 65(Suppl 5):13–18
for their assistance in data collection.
Moskowitz H (1973) Laboratory studies of the effects of alcohol on
some variables related to driving. J Saf Res 5:185–199
Mumford GK, Evans SM, Fleishaker JC, Griffiths RR (1995)
Alprazolam absorption kinetics affects abuse liability. Clin
Neutel CI (1995) Risk of traffic accidents injury after prescription for
Barbone F, McMahon AD, Davey PG, Morris AD, Reid IC, McDevitt
a benzodiazepine. Ann Epidemiol 5:239–244
DG, MacDonald TM (1998) Association of road-traffic accidents
Neutel I (1998) Benzodiazepine-related traffic accidents in young and
with benzodiazepine use. Lancet 352:1331–1336
elderly drivers. Hum Psychopharmacol Clin Exp 13:S115–S123
Bertz RJ, Kroboth PD, Kroboth FJ, Reynolds IJ, Salek F, Wright CE,
O’Hanlon JF (1984) Driving performance under the influence of
Smith RB (1997) Alprazolam in young and elderly men:
drugs: rationale for, and application of, a new test. Br J Clin
sensitivity and tolerance to psychomotor, sedative and memory
effects. J Pharmacol Exp Ther 281:1317–1329
O’Hanlon JF, Ramaekers JG (1995) Antihistamine effects on actual
Borkenstein RF (1974) The role of the drinking driver in traffic
driving performance in a standard test: a summary of Dutch
accidents, the Grand Rapids study. Blutalkohol 11
experience, 1989–94. Allergy 50:234–242
Busto UE, Kaplan HL, Wright CE, Gomez-Mancilla B, Zawertailo L,
O’Hanlon JF, Vermeeren A, Uiterwijk MM, van Veggel LM,
Greenblatt DJ, Seller EM (2000) A comparative pharmacokinetic
Swijgman HF (1995) Anxiolytics’ effects on the actual driving
and dynamic evaluation of alprazolam sustained-release, broma-
performance of patients and healthy volunteers in a standard-
zepam, and lorazepam. J Clin Psychopharmacol 20:628–635
ized test. An integration of three studies. Neuropsychobiology
Curran HV (1986) Tranquillising memories: a review of the effects of
benzodiazepines on human memory. Biol Psychol 23:179–213
Ramaekers JG (2003) Antidepressants and driver impairment: empir-
Eller MG, Della-Coletta AA (1990) Absence of effect of food on
ical evidence from a standard on-the-road test. J Clin Psychiatry
alprazolam absorption from sustained release tablets. Biopharm
Ramaekers JG, Kuypers KPC (2006) Acute effects of 3,4-
Ellinwood EH Jr, Heatherly DG, Nikaido AM, Bjornsson TD, Kilts C
methylenedioxymethamphetamine (MDMA) on behavioral
(1985) Comparative pharmacokinetics and pharmacodynamics of
measures of impulsivity: alone and in combination with
lorazepam, alprazolam and diazepam. Psychopharmacology
alcohol. Neuropsychopharmacology 31:1048–1055
Ramaekers JG, Louwerens JW, Muntjewerff ND, Milius H, de Bie A,
Fillmore MT, Rush CR, Hays L (2002) Acute effects of oral cocaine
Rosenzweig P et al (1999) Psychomotor, cognitive, extrapyrami-
on inhibitory control of behavior in humans. Drug Alcohol
dal, and affective functions of healthy volunteers during
treatment with an atypical (amisulpride) and a classic (haloper-
Fleishaker JC, Phillips JP, Eller MG, Smith RB (1989) Pharmacoki-
idol) antipsychotic. J Clin Psychopharmacol 19:209–221
netics and pharmacodynamics of alprazolam following single and
Rey A (1964) L’examen clinique en psychologie. Presses Universi-
multiple oral doses of a sustained-release formulation. J Clin
Rickels K (2004) Alprazolam extended-release in panic disorder.
Glue P, Fang A, Gandelman K, Klee B (2006) Pharmacokinetics of an
extended release formulation of alprazolam (Xanax XR) in
Robbe HW, O’Hanlon JF (1995) Acute and subchronic effects of
healthy normal adolescent and adult volunteers. Am J Ther
paroxetine 20 and 40 mg on actual driving, psychomotor
performance and subjective assessments in healthy volunteers.
Greenblatt DJ, Wright CE (1993) Clinical pharmacokinetics of
alprazolam. Therapeutic implications. Clin Pharmacokinet
RxList (2005) Top 200 prescriptions for 2005 by number of US
Scavone JM, Greenblatt DJ, Goddard JE, Friedman H, Harmatz JS,
Vermeeren A, Jackson JL, Muntjewerff ND, Quint PJ, Harrison EM,
Shader RI (1992) The pharmacokinetics and pharmacodynamics
O’Hanlon JF (1995) Comparison of acute alprazolam (0.25, 0.50
of sublingual and oral alprazolam in the post-prandial state. Eur J
and 1.0 mg) effects versus those of lorazepam 2 mg and placebo
on memory in healthy volunteers using laboratory and telephone
Smith RW, Kroboth PD (1987) Influence of dosing regime non
alprazolam and metabolite serum concentrations and tolerance to
Vermeeren A, Riedel WJ, van Boxtel CJ, Darwish M, Paty I, Patat A
sedative and psychomotor effects. Psychopharmacology 93:105–
(2002) Differential residual effects of zaleplon and zopiclone on actual
driving: a comparison with a low dose of alcohol. Sleep 25:224–231
Smith RB, Kroboth PD, Vanderlugt JT, Phillips JP, Juhl RP (1984)
Verster JC, Volkerts ER (2004a) Antihistamines and driving ability:
Pharmacokinetics and pharmacodynamics of alprazolam after
Evidence from on-the-road driving studies during normal traffic.
oral and iv administration. Psychopharmacology 84:452–456
Subhan Z, Harrison C, Hindmarch I (1986) Alprazolam and
Verster JC, Volkerts ER (2004b) Clinical pharmacology, clinical
lorazepam single and multiple-dose effects on psychomotor skills
efficacy, and behavioral toxicity of alprazolam: a review of the
and sleep. Eur J Clin Pharmacol 29:709–712
Van Laar MW, Volkerts ER, Van Willigenburg APP (1991) Thera-
Verster JC, Volkerts ER, Verbaten MN (2002) Effects of alprazolam
peutic effects and effects on actual driving performance of
on driving ability, memory functioning and psychomotor
chronically administered buspirone and diazepam in anxious
performance: a randomized, placebo-controlled study. Neuro-
outpatients. J Clin Psychopharmacol 12:86–95
Vermeeren A (2004) Residual effects of hypnotics: epidemiology and
Verster JC, Veldhuijzen DS, Volkerts ER (2005) Is it safe to drive a car
clinical implications. CNS Drugs 18:297–328
when treated with anxiolytics? Evidence from on-the-road driving
Vermeeren A, De Gier JJ (1995) Methodological guidelines for
studies during normal traffic. Curr Psychiatry Rev 1:215–225
experimental research in drugs and driving: accomplishments
Vuurman EF, Uiterwijk MM, Rosenzweig P, O’Hanlon JF (1994)
and future needs. In: Krüger HP, Kohnen R, Schoch H (eds)
Effects of mizolastine and clemastine on actual driving and
Medicamente im Strassenverkehr: Auftreten, Risiken Konse-
psychomotor performance in healthy volunteers. Eur J Clin
quenzen. Gustav Fisher Verlag, Stuttgart, pp 49–59
Journal of Xinjiang University(Natural Science Edition)LIN Hui-qiu, MENG Ji-xiang † , TIAN Ying-zhi( College of Mathematics and Systems Science, Xinjiang University, Urumqi, Xinjiang 830046, China )A subset S ⊂ E ( G ) is called a 4-restricted-edge-cut of G , if G − S is disconnected and everycomponent contains at least 4 vertices. The minimum cardinality over all 4-restricted-edge-c
I N S T I T U T L A C O N F É R E N C E H I P P O C R A T E Cas Clinique mars 2009 ÉDITORIAL L’Institut la Conférence Hippocrate, grâce au mécénat du groupe de recherche SERVIER,contribue à la formation des jeunes médecins, et en particulier à la préparation au concoursde l’Internat depuis 1982. Cette démarche repose sur deux éléments clés : une méthode detra
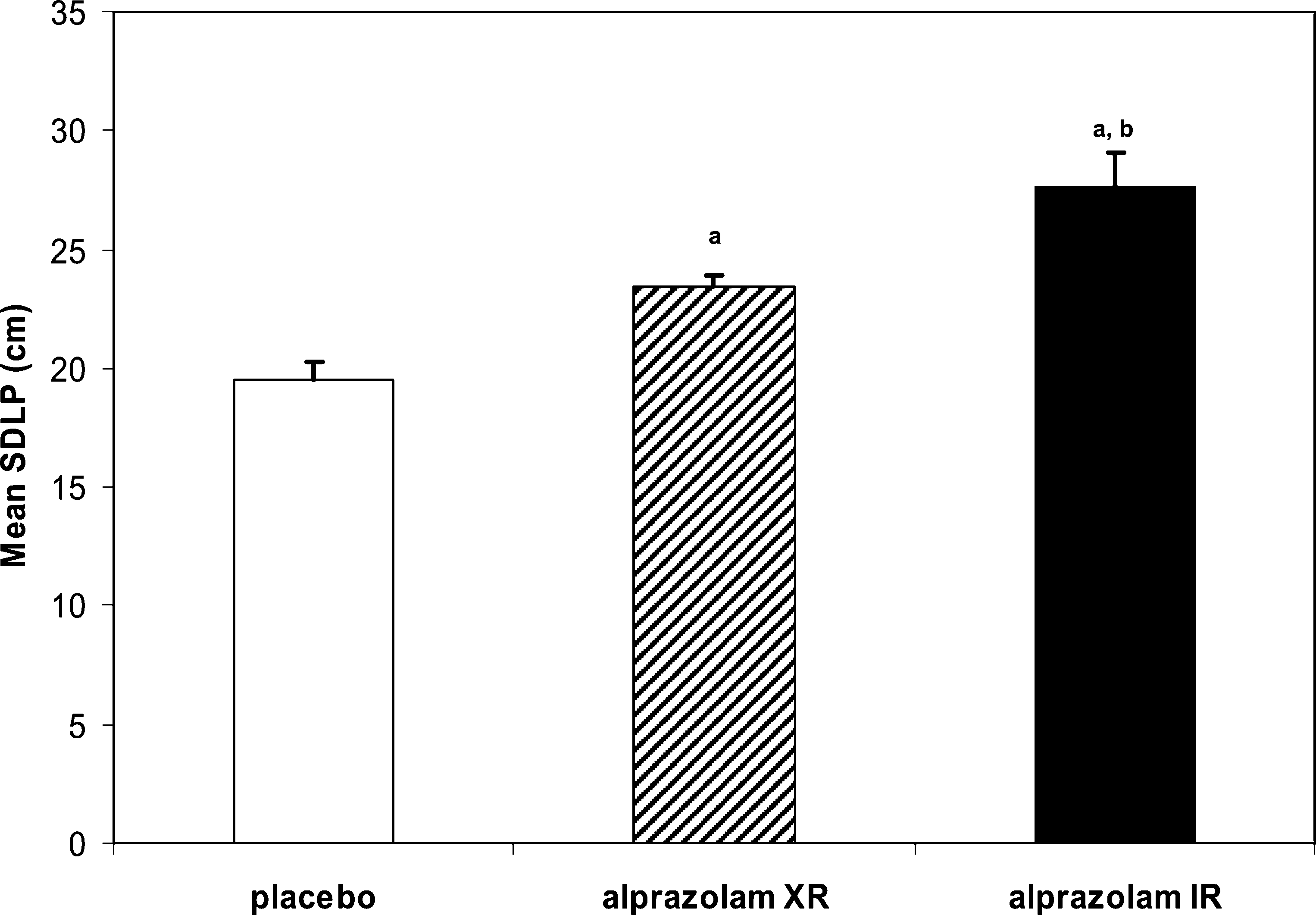 Fig. 1 Mean (±SE) StandardDeviation of Lateral Position(SDLP) in each drug condition.
Fig. 1 Mean (±SE) StandardDeviation of Lateral Position(SDLP) in each drug condition.