Tadalafil entfaltet seine Wirkung über eine selektive Hemmung der PDE5, wodurch die Konzentration von cGMP im glatten Muskelgewebe stabil bleibt. Diese biochemische Modulation resultiert in einer langanhaltenden Relaxation der Gefäßwände. Der Wirkstoff wird nach oraler Einnahme effizient resorbiert, mit einer Bioverfügbarkeit von rund 80 %. Seine Halbwertszeit von bis zu 36 Stunden ist innerhalb dieser Substanzklasse außergewöhnlich. Abgebaut wird er in der Leber, hauptsächlich durch CYP3A4, mit anschließender biliärer Exkretion. Typische unerwünschte Wirkungen entstehen durch eine verstärkte Vasodilatation, etwa Kopfschmerzen oder Flush. Pharmakologisch wird cialis generika vor allem durch die verlängerte Wirkungsdauer charakterisiert.
Health.uml.edu
Mayo Clin Proc, March 2001, Vol 76 Pellagra in 2 Homeless Men Pellagra in 2 Homeless Men STEFAN G. KERTESZ, MD Pellagra is a nutritional disease with cutaneous, gas- diet. Appropriate suspicion for a diagnosis of pellagra trointestinal, and neuropsychiatric manifestations. Be- requires attention to a combination of socioeconomic and cause of the diversity of pellagra’s signs and symptoms, behavioral risk factors for nutritional deficiency. The diagnosis is difficult without an appropriate index of suspi- combination of homelessness, alcohol abuse, and failure to cion. Untreated, pellagra is fatal. Two cases of pellagra in eat regularly—particularly, failure to make use of shelter- contemporary homeless people are described. Complete based meal programs—may identify people at special risk evaluation supported a clinical diagnosis of pellagra after in contemporary settings. exclusion of other possibilities. Signs and symptoms re- solved after institution of niacin therapy and change in Mayo Clin Proc.2001;76:315-318
Pellagra, a disease primarily due to niacin deficiency, tobacco. He had lived on the street and avoided shelters for
was epidemic in the United States before 1950. Al-
4 months. Examination revealed bronze-colored skin with
though contemporary medical literature focuses on the his-
rare scale formation, poor dentition, and low-grade fever.
tory of its eradication,1 some reports suggest that pellagra
Initial laboratory studies showed the following: hematocrit,
continues to occur2 but remains underappreciated, resulting
33.8%; mean corpuscular volume, 104 fL; normal leuko-
in delayed diagnosis. Two series from Japan describe 28
cyte and platelet counts; normal renal function test results;
patients who died of undiagnosed pellagra and underscore
serum alanine aminotransferase, 76 U/L; serum aspartate
the importance of identifying populations at special risk.3,4
aminotransferase, 126 U/L; albumin, 3.5 g/dL; total pro-
To my knowledge, no report to date has described pella-
tein, 5.6 g/dL; and erythrocyte sedimentation rate, 23 mm/1
gra in contemporary homeless people, despite the fact that
h. Chest radiograph, electrocardiogram, and serial creatine
the homeless are subject to relevant vulnerabilities of alco-
kinase determinations were normal. Additional work-up
holism, social dislocation, and irregular access to food.
included the following tests, the results of which were
This article describes 2 cases of pellagra in this population.
normal: serum thyrotropin, cortisol, vitamin B , folate,
iron studies, and rapid plasma reagin test; stool cultures and
examinations for ova and parasites; sequential blood cul-
tures for bacteria, mycobacteria, and fungi; serum histo-
A 58-year-old homeless man was admitted to a Boston
plasma antigen assay; serum gastrin and vasoactive intesti-
hospital in October 1998 with chest pain and fatigue. Re-
nal peptide levels; 24-hour urinary 5-hydroxyindoleacetic
view disclosed multiple complaints, including fever, night
acid, catecholamines, vanillylmandelic acid, and meta-
sweats, 4.5-kg weight loss, a burning sensation in the
nephrines; and computed tomography of the torso and jaw.
mouth, nausea, vomiting, diarrhea involving watery, large-
Two teeth were extracted. The symptoms improved
volume movements several times daily, cutaneous burning
slightly without specific intervention, and the patient was
sensations, increased skin pigmentation, cough, and pro-
discharged; a multivitamin, thiamine, and folate were pre-
nounced emotional lability over the preceding months.
scribed. At outpatient follow-up 1 week later, the patient
The patient’s history was unremarkable, including nega-
reported minimal improvement. A diagnosis of nutritional
tive purified protein derivative and negative serum human
deficiency was entertained. A dietary history revealed that
immunodeficiency virus test results. The patient reported
the patient had subsisted on 2 to 3 alcoholic beverages and
drinking 2 or 3 alcoholic beverages per day as well as using
a daily snack, usually corn chips, for 4 months. He hadavoided homeless shelters and shelter-based meal pro-grams. Information obtained later suggested that the patient
From the Boston Health Care for the Homeless Program and the
had a history of bipolar illness, although neither mania nor
Section of General Internal Medicine, Boston Medical Center, Bos-
depression was evident at the time of admission. A pre-
sumed diagnosis of pellagra led to the institution of supple-
Address reprint requests and correspondence to Stefan G. Kertesz,
mental niacin, 100 mg orally twice daily; the patient also
MD, Section of General Internal Medicine Research Unit, 91 E Con-cord St, Suite 200, Boston, MA 02118 (e-mail: skertesz@bu.edu).
obtained regular meals from a shelter. All symptoms, in-
2001 Mayo Foundation for Medical Education and ResearchMayo Clin Proc, March 2001, Vol 76 Pellagra in 2 Homeless Men
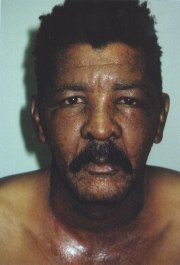
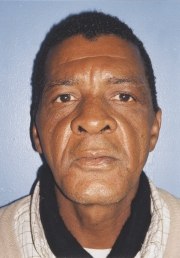
Figure 1. Patient 2. Left, at time of presentation. Two weeks into the course of the illness, cutaneousweeping, edema, erythema, fissuring, and scale were noted over the ears, face, and collar area. Right, 1year later.
cluding cutaneous burning sensations, rash, diarrhea, and
diagnostic considerations included photodermatitis, actinic
mood alteration, resolved within 2 weeks.
dermatitis, and pellagra. The patient was prescribed a mul-tivitamin, niacin (100 mg orally daily), and triamcinolone
cream; the patient reported that his rash resolved over the
A 55-year-old homeless man presented to a shelter
next few weeks. A photograph obtained 1 year later docu-
clinic in July 1998 with several days of a weeping eczema-
mented complete resolution (Figure 1, right).
tous rash of the face, ears, and neck (Figure 1, left). Physi-
After resolution of his symptoms, the patient reported
cal examination demonstrated extensive cutaneous weep-
that, for several months preceding his illness, he had
ing, edema, erythema, fissuring, and scale over the ears,
missed meals for up to 4 days at a time, subsisting on
face, collar area, and forearms. He had no other known
coffee, donuts, and alcohol, while generally avoiding
medical conditions. He received topical corticosteroids and
homeless shelters. He recalled a burning sensation in his
antibiotics for a diagnosis of allergic contact dermatitis
mouth, increased psychological irritability, and continuous
abdominal upset without diarrhea, all of which subsided
The rash did not abate after 1 week, and the patient was
with vitamin therapy and regular meals. The distribution of
referred to a dermatology service. Evaluation included nor-
the patient’s rash, the nonspecific dermatological work-up,
mal blood cell counts, liver function test results, urinalysis,
and the resolution of all symptoms with niacin therapy
and urine porphyrins. A serum antinuclear antibody assay
were judged to represent a diagnosis of pellagra.
was positive with a speckled pattern on Hep2 cells at a titerof 1:160, but there were no joint, renal, or hematologic
abnormalities. Biopsy of the left preauricular skin showed
This report describes pellagra in 2 homeless men, with
compact orthokeratosis, mild epidermal hyperplasia, focal
diagnosis based on clinical presentation, negative or non-
spongiosis, mild to moderate superficial perivascular
specific findings after extensive evaluation, and resolution
lymphohistiocytic infiltrates with occasional eosinophils
of cutaneous, gastrointestinal, and psychiatric symptoms
and neutrophils, and mild papillary dermal fibrosis; these
after change in food intake and therapy with niacin. A
findings were nonspecific. The dermatology service’s final
standard textbook recommends diagnosis based on clinical
Mayo Clin Proc, March 2001, Vol 76 Pellagra in 2 Homeless Men
assessment and response to therapy because most postu-
vitamins, surveys have had difficulty identifying an in-
lated laboratory indicators, including urinary nicotinamide
creased prevalence of niacin deficiency among alcoholics
and serum niacin levels, have not proved reliable5-7; one
since the fortification of flour began after World War II.18,19
assay involving high-performance liquid chromatography
The pre-1950 case literature identifying an association be-
is not commonly available.8 In the absence of definitive
tween alcoholism and pellagra20 did not describe patients’
laboratory results, this report relied on clinical diagnosis.
socioeconomic status. Nevertheless, indigence and alco-
A functional deficiency of niacin plays a central role in
holism together may pose special nutritional risk. In 1923,
the pathophysiology of pellagra; however, contemporary
Shattuck21 suggested that dietary inadequacy due to poverty
research has shown that an interplay of niacin and other
could account for the development of pellagra among alco-
metabolic factors actually determines whether the disease
holics. Of 15 alcoholics with pellagra in the 1977 series by
will develop in a given person.9 Coexistent deficiencies of
Spivak and Jackson,2 14 were classified as indigent.
riboflavin and pyridoxine, although unmeasured in our
Homelessness does confer an increased risk of dietary
inadequacy. Contemporary homeless people frequently
Although both patients fulfilled diagnostic criteria
miss meals and have substantial rates of dietary insuffi-
based on clinical manifestations in 3 organ systems, this
ciency when evaluated by nutritional surveys of vitamin
diagnostic approach would overlook other cases. Only 22%
intake, although few studies have assessed niacin in par-
of patients in one series presented with symptoms in 3
ticular.22-25 Anthropometric studies provide additional evi-
systems.2 For this reason, identification of epidemiological
dence of malnutrition in homeless people, but the absolute
rate of reported nutritional deficiency disease in this popu-
A search of the MEDLINE database identified no previ-
lation remains low.13,26 At least one study found shelter-
ous reports of pellagra in homeless people. Given the sub-
based meal programs to be reasonably well balanced with
stantial literature describing delayed diagnosis leading to
respect to protein and carbohydrate,27 and access to free
patient deaths,2-4 the occurrence of this disease in the con-
food sources is likely to prevent malnutrition among the
temporary homeless may be underappreciated. The home-
less population has grown during the past decade, with
Because both patients in this report had avoided home-
estimates of the homeless ranging from 440,000 to 842,000
less shelter-based meal programs for several months before
people during any given week in 1996.11 Although avail-
the development of symptoms, they are likely to have been
able studies identify the broad range of medical conditions
especially susceptible to nutritional deficiency.
affecting homeless people,12,13 the published literature hasonly rarely described the specific nutritional deficiency
diseases to which homeless persons are subject.14 For this
The present cases, diagnosed after delay, underscore a
reason, pellagra may continue to go unrecognized unless
contemporary dilemma. A fatal but easily treated disease is
physicians develop an index of suspicion for its occurrence.
readily overlooked because of its rarity. Neither a history of
Pellagra’s manifestations include a rash over sun-ex-
alcohol use nor homelessness alone has a strong positive
posed areas that develops in spring or summer. The simul-
predictive value for a diagnosis of pellagra. Homelessness
taneous occurrence of a severe rash of the face, forearms,
coupled with alcoholism in patients who do not obtain
and collar region, as was seen in patient 2, suggests classic
meals from shelter-based meal programs, however, appears
pellagra. But the literature contains reports of more subtle
to identify a group at special risk.
findings, including diffuse, mild hyperpigmentation,2 aswas seen in patient 1. The literature also documents the
I gratefully acknowledge the editorial advice of Drs Mark
occurrence of pellagra without rash (“pellagra sine pella-
Moskowitz, John Noble, and James O’Connell in the preparationof this article and the assistance of Dr James O’Connell in obtain-
gra”), affecting 15% of patients in a compilation of 4121
cases.15 Patients without rash may die of pellagra’s neuro-logic sequelae.4 Gastrointestinal manifestations include not
only diarrhea but also glossitis, nausea, vomiting, and post-
Rajakumar K. Pellagra in the United States: a historical perspec-
prandial discomfort.16 Neuropsychiatric manifestations
tive. South Med J. 2000;93:272-277.
vary and can include cognitive dysfunction, memory im-
Spivak JL, Jackson DL. Pellagra: an analysis of 18 patients and areview of the literature. Johns Hopkins Med J. 1977;140:295-309.
pairment, insomnia, anxiety, depression, acute psychosis,
Ishii N, Nishihara Y. Pellagra encephalopathy among tuberculous
seizures, ataxia, and spastic paraparesis.3,17
patients: its relation to isoniazid therapy. J Neurol Neurosurg Psy-
Whether the nutritional vulnerability of these 2 patients
Ishii N, Nishihara Y. Pellagra among chronic alcoholics: clinical
might best be attributed to alcohol use or to homelessness
and pathological study of 20 necropsy cases. J Neurol Neurosurg
itself can be debated. Despite alcohol’s effect on many
Mayo Clin Proc, March 2001, Vol 76 Pellagra in 2 Homeless Men
Wilson JD. Vitamin deficiency and excess. In: Fauci AS,
Spies TD. Niacinamide malnutrition and pellagra. In: Joliffe N,
Braunwald E, Isselbacher KJ, et al, eds. Harrison’s Principles of
Tisdall FF, Cannon PR, eds. Clinical Nutrition. New York, NY: PB
Internal Medicine. Vol 1. 14th ed. New York, NY: McGraw-Hill Co,
Serdaru M, Hausser-Hauw C, Laplane D, et al. The clinical spectrum
Field H Jr, Melnick D, Robinson WD, Wilkinson CF Jr. Studies on
of alcoholic pellagra encephalopathy: a retrospective analysis of 22
the chemical diagnosis of pellagra (nicotinic acid deficiency). J
cases studied pathologically. Brain. 1988;111(pt 4):829- 842. Clin Invest. 1941;20:379-386.
Figueroa WG, Sargent F, Imperiale L, Morey GR, Paynter CR,
Sauberlich HE. Newer laboratory methods for assessing nutri-
Vorhaus LJ. Lack of avitaminosis among alcoholics: its relation to
ture of selected B-complex vitamins. Annu Rev Nutr. 1984;4:377-
fortification of cereal products and the general nutritional status of
the population. J ClinNutr. 1953;1:179-199.
Dillon JC, Malfait P, Demaux G, Foldi-Hope C. The urinary me-
Neville JN, Eagles JA, Samson G, Olson RE. Nutritional status of
tabolites of niacin during the course of pellagra [in French]. Ann
alcoholics. Am J ClinNutr. 1968;21:1329-1340.
Klauder JV, Winkelman NW. Pellagra among chronic alcoholic
Bapurao S, Krishnaswamy K. Vitamin B6 nutritional status of
addicts: a clinical and laboratory study. JAMA. 1928;90:364-371.
pellagrins and their leucine tolerance. Am J Clin Nutr. 1978;31:
Shattuck GC. Factors apparently influencing the development of
pellagra in Massachusetts. Boston Med Surg J. 1923;188:889-891.
Carpenter KJ, Lewin WJ. A reexamination of the composition of
Burt MR, Cohen BE. America’s Homeless: Numbers, Characteris-
diets associated with pellagra. J Nutr. 1985;115:543-552. tics, and Programs that Serve Them. Washington, DC: Urban
Burt MR, Aron L. America’s Homeless II: Populations and Ser-vices. Washington, DC: Urban Institute; 2000. Available at:
Silliman K, Yamanoha MM, Morrissey AE. A survey of the nutri-
www.urbaninstitute.org/housing/homeless/numbers/index.htm.
tional status of homeless adults in rural Northern California [ab-
Accessibility verified February 8, 2001.
stract]. J Am Diet Assoc. 1995;95(suppl):A92.
Ferenchick GS. The medical problems of homeless clinic patients:
Wolgemuth JC, Myers-Williams C, Johnson P, Henseler C. Wasting
a comparative study. J Gen Intern Med. 1992;7:294-297.
malnutrition and inadequate nutrient intakes identified in a multi-
Wright JD, Weber E. Homelessness and Health. Washington, DC:
ethnic homeless population. J Am DietAssoc. 1992;92:834-839.
McGraw-Hill’s Healthcare Information Center; 1987:169.
Wiecha JL, Dwyer JT, Dunn-Strohecker M. Nutrition and health
Darnton-Hill I, Truswell AS. Thiamin status of a sample of home-
services needs among the homeless. Public Health Rep. 1991;106:
less clinic attenders in Sydney. Med J Aust. 1990;152:5-9.
Gillman J, Gillman T. Perspectives in Human Malnutrition; A
Gelberg L, Stein JA, Neumann CG. Determinants of undernutrition
Contribution to the Biology of Disease From a Clinical and Patho-
among homeless adults. Public Health Rep. 1995;110:448-454. logical Study of Chronic Malnutrition and Pellagra in the African.
Carillo TE, Gilbride JA, Chan MM. Soup kitchen meals: an obser-
New York, NY: Grune & Stratton; 1951.
vation and nutrient analysis. J Am Diet Assoc. 1990;90:989-991.
Guidance for Influenza: Taking Care of a Sick Person in Your Content source: Centers for Disease Control and Prevention This document provides interim guidance and will be updated as needed Introduction Influenza can cause a wide range of symptoms, including fever, cough, sore throat, body aches, headache, chills and fatigue. Influenza can vary in severity from mil
The Model Formulation Count what is countable, measure what is measurable, and what is not measurable, make measurable. 4.1 The Overall Process In using any kind of analytical or modeling approach for attacking a problem, there are five major steps:1) Understanding the real problem. 2) Formulating a model of the problem. 3) Gathering and generating the input data for the model (e.g., pe
 Mayo Clin Proc, March 2001, Vol 76
Mayo Clin Proc, March 2001, Vol 76