Tadalafil entfaltet seine Wirkung über eine selektive Hemmung der PDE5, wodurch die Konzentration von cGMP im glatten Muskelgewebe stabil bleibt. Diese biochemische Modulation resultiert in einer langanhaltenden Relaxation der Gefäßwände. Der Wirkstoff wird nach oraler Einnahme effizient resorbiert, mit einer Bioverfügbarkeit von rund 80 %. Seine Halbwertszeit von bis zu 36 Stunden ist innerhalb dieser Substanzklasse außergewöhnlich. Abgebaut wird er in der Leber, hauptsächlich durch CYP3A4, mit anschließender biliärer Exkretion. Typische unerwünschte Wirkungen entstehen durch eine verstärkte Vasodilatation, etwa Kopfschmerzen oder Flush. Pharmakologisch wird cialis generika vor allem durch die verlängerte Wirkungsdauer charakterisiert.
Img840.imageshack.us
INTERNATIONAL JOURNAL OF GERIATRIC PSYCHIATRY
Int J Geriatr Psychiatry 2005; 20: 1038–1045.
Published online in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/gps.1393
The utility of EEG in dementia: a clinical perspective
Dimitrios Adamis1, Sunita Sahu2 and Adrian Treloar2,3
1Deptartment of Ageing and Health, Guy’s and St Thomas’ NHS Foundation Trust, London, UK2Old Age Psychiatry, Oxleas NHS Trust, Memorial Hospital, Shooter Hill, London, UK3Old Age Psychiatry, The Institute of Psychiatry, London, UK
Despite being simple and cheap, the EEG is not often used in clinical practice.
Literature search using PUBMED and Medline.
Quantitative EEG can help to identify mild dementia and mild cognitive impairment and can increase diagnostic
accuracy when used with other imaging techniques. EEG helps differentiate organic from functional brain disease and pre-dict response to cholinesterase inhibitors and is central in the diagnosis of Creutzfeldt Jacob disease. The accuracy of EEGmay be greater than that of CT or MRI scans alone. Discussion
Quantitative EEG may save on specialist interpretation time and enable more routine use of EEG in diagnosis
and care. More widespread use of EEG’s is indicated. Agreement on the parameters that are best measured on qEEG is stillawaited. Copyright # 2005 John Wiley & Sons, Ltd.
key words — electroencephalography; dementia; psychiatric services; review
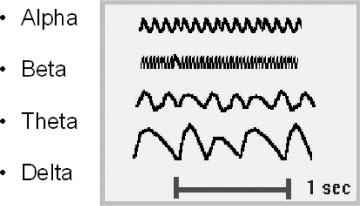
by sleep, activity, medication and age. Delta waveshave frequencies below 4 Hz and may be regular or
Few patients with dementia have biological brain tests
irregular. Diffuse delta waves are normal in sleeping
apart from CT and MRI scans. EEG provides informa-
adults and children, but abnormal in awake adults.
tion about the physiological state of the brain both in
They are the most common focal pathological wave-
health and disease. Quantitative EEG (qEEG) uses
form. Theta waves (4–7 Hz), are transiently present in
computer software to provide topographic analysis
15% of the normal population. Alpha waves (8–
of brain activity, allowing abnormalities to be
13 Hz) are normal in awake adults with closed eyes.
recorded on the outline of a head (Brain Electrical
Prominent in occipital channels they are symmetrical
Activity Mapping). Techniques such as Coherence
and should disappear when the eyes are open. Beta
analysis (Leocani and Comi, 1999) and Power Spectra
waves (14 Hz and above) are normally present when
analysis (Signorino et al., 1995) allow objective data
the eyes are either open or closed. They are prominent
to be provided without reliance upon subjective visual
over the fronto-central regions and are increased by
benzodiazepines, barbiturates, alcohol and anxiety. (See Figure 1).
Activation procedures are used in epilepsy in particu-
lar and include sleep deprivation, hyperventilation
We searched Medline and Pubmed for recent publica-
and photic stimulation. The EEG may be affected
tions (1996–04) using key words Electroencephalo-graphy (EEG) and one of dementia, Alzheimer’s,Huntingdon’s, AIDS, HIV, Multi-Infarct, Creutz-
*Correspondence to: Dr A. Treloar, Room 19 Memorial Hospital,
feldt-Jacob, Fronto-Temporal, Lewy body and Parkin-
Shooters Hill, London SE18 3RZ, UK. Tel: 020 8836 6407. Fax:020 8836 6381. E-mail: Adrian.Treloar@oxleas.nhs.uk
son’s. We reviewed papers which suggested that EEG
Copyright # 2005 John Wiley & Sons, Ltd.
nitively impaired individuals with elevated CSF tauprotein levels. Lehtovirta et al. (2000) found thatAD patients carrying the Apolipoprotein sigma4allele had more pronounced slow wave activity thanAD patients without the sigma4 allele. Examiningthe ApoE epsilon 4 allele, Jelic et al. (1997) foundthat ApoE epsilon4 allele does not influence EEGslowing but it was associated with a decrease in func-tional connectivity.
EEG as a predictor of dementia’s progression
Berg et al. (1984) found that EEG did not predict pro-gression of dementias. Subsequently however, Helkalaet al. (1991) found that those with abnormal EEG inthe early stages of dementia had greater declines inpraxis, more extrapyramidal symptoms and a greater
might be a useful diagnostic aid, or predict response
risk for institutionalisation. Nobili et al. (1999) using
to treatment. We then included relevant citations from
qEEG in AD patients found that the loss of activities in
daily living was predicted by delta power in eitherhemisphere, and incontinence predicted by alphapower on the right side. Claus et al. (1998a) also found
slowing on qEEG to predict cognitive and functional
The EEG identifies non-specific brain dysfunction in
decline in AD. In another study (Claus et al., 1998b)
Alzheimer’s disease. (Robinson et al., 1994). Can the
found that mortality in patients with early AD was pre-
EEG help to identify normal ageing form early
dicted by a decrease in alpha and beta activity on spec-
dementia or do changes only occur once the diagnosis
tral EEG. Lopez et al. (1997) found that abnormal
is clear? Anecdotal evidence suggests that the EEG is
EEG at entry was associated with worse outcomes
used more often as part of a diagnostic process in
during follow up. Edwards-Lee et al. (2000) also
younger patients, to differentiate functional illness
found that EEG was worse in those with psychosis
from organic early AD. Many studies (summarised
in dementia. Jelic et al. (2000) studied a sample of
in Table 1) have shown AD to relate to EEG. As well
subjects with mild cognitive impairment who they fol-
as distinguishing functional from organic disease
lowed for 21 months using EEG. They found that the
EEG can also distinguish very mild cognitive impair-
important predictors for progression to AD were alpha
ment from normal ageing. Indeed EEG may be more
and theta relative power and mean frequency from left
accurate than MRI or CT. Quantitative analysing
temporal-occipital region which classified 85% of
techniques, may increase the sensitivity of the EEG
mild cognitive impaired subjects correctly. Therefore
so that it can be used to differentiate normal aging
EEG slowing early on in AD, does appear to predict
from early dementia. But there is yet a lack of clarity
about which are the best qEEG markers to identifymildly cognitively impaired subgroups that later pro-
gress to clinically obvious AD. It may be that EEGand neuroimaging techniques used together (espe-
The literature on ability of EEG to distinguish AD
cially with rCBF) can increase diagnostic accuracy.
from MID is conflicting. Erkinjuntti et al. (1988)compared AD patients to MID patients and found that
the degree of diffuse abnormalities and the mean fre-quency of background activity did not differ between
EEG also has been used in research studies of Alzhei-
the AD and MID groups. But Leuchter et al. (1987)
mer’s disease in conjunction with biological markers
reported that 92% of subjects with either AD or
like Apolipoprotein E and tau protein. Jelic et al.
MID were accurately classified using discriminate
(1998a) found CSF (Cerebrospinal fluid) tau protein
analysis of both EEG frequency and coherence.
to be related to the EEG alpha/delta ratio. No such
Further studies with EEG tried to resolve this pro-
correlation was found in healthy controls or mild cog-
blem. d’Onofrio et al. (1996) suggested that qEEG
Copyright # 2005 John Wiley & Sons, Ltd.
Int J Geriatr Psychiatry 2005; 20: 1038–1045.
Studies of EEG use in diagnosing Alzheimer’s dementia
Studies of moderate to severe dementia; Increased slow activity
and decreased mean frequency correlate with cognitive impair-
Weiner and Schshrer (1956), Coben et al.
Severity of EEG abnormalities and cognitive impairment
correlated. Correlation between cognitive deficit and both theta increase andconcomitant fast beta activity decrease.
Brenner et al. (1986, 1989), Adler et al.
Differentiation from depression with 69%–84% accuracy
Increased global theta power decreased left temporal alphacoherence and decreased interhermispheric thetas coherence inAD patients compared with cognitively normal depressedcontrols. The left temporal alpha coherence and global thetapower allowed an identification of AD patients with a sensitivityof 87% and a specificity of 77%.
Pijnenburg et al. (2004), Prichep et al.
Synchronisation likelihood differentiates AD from subjective
memory impairment. Beta synchronisation helps to distinguish
AD from controls and Mild Cognitive Impairment.
Increase in theta power present in earlier stages of AD. Reduced beta band synchronisation in early and mild AD. Resting state alpha dipolarity (D(alpha) distinguishes early ADfrom normal controls. Topography of beta and delta, delta activity, and amplitude ofdelta activity gave a sensitivity and specificity of over 90%discriminating AD patients from normal subjects. Temporo-parietal coherence a discriminate variable togetherwith alpha and theta relative power between AD patients andcontrols giving a 77.8% sensitivity and 100% specificity.
Proposed the use of power ratios (ratios between fast and slow
Visually assessed EEG, found a high specificity of 89.1% and a
sensitivity of 44.6% to diagnose AD in a memory clinic.
Brenner et al. (1986), Dunkin et al.
Good correlations between EEG and psychometric tests.
(1995), Strijers et al. (1997), Rodriguez
Eight-degree scale correlated with the severity of cognitive
impairment 19 channel EEG, mild dementia (n ¼ 17) and
Generalised frequency [È] highly correlated with MMSE scoresand performance IQ scores of the Japanese WAIS.
Early onset AD have a different pattern of spectral parameters
qEEG was more accurate (81–84%) than MRI (72%) in AD
patients diagnosed using the CAMDEX. Noted incompleteoverlap of the two groups suggesting that if used together,accuracy would be further enhanced.
Muller et al. (1997a), Pozzi et al. (1996)
qEEG better correlated with clinical severity than SPECT.
Montplaisir et al. (1996), Claus et al.
AD patients with lower frontal perfusion were no different on
qEEG from normal subjects but the usefulness of qEEG for the
diagnosis of dementia is restricted to a subgroup of patient with aSPECT pattern of parietal blood hypoperfusion. REM sleep on qEEG more useful than SPECT in mild tomoderate AD. EEG related to CT scans to some degree.
qEEG alone had an accuracy of 77% for the whole group(normal vs AD) and of 69% in mild AD. When qEEG and rCBFwere used together, accuracy was 88.3%. The sensitivity of bothprocedures was 88% and specificity was 89%. rCBF and qEEGappear to be the best predictors of AD severity.
Copyright # 2005 John Wiley & Sons, Ltd.
Int J Geriatr Psychiatry 2005; 20: 1038–1045.
is a useful ancillary test to differentiate MID from
EEG in In Lewy Body (LBD) and Parkinson’s
AD. A more recent study by Moretti et al. (2004) also
concluded that analysis of the alpha frequency and
The abnormalities reported in Parkinson’s disease
power can discriminate mild AD from Vascular
dementia consist of non-specific diffuse changes such
dementia and normal elderly subjects. Sato et al.
as slowing of background rhythms posteriorly and an
(1996) found differences in EEG component waves
increase in theta and delta activity (Brenner, 1993).
between normal and MID subjects. Coherence studies
Wszolek et al. (1998) studied patients with rapidly
have shown that long distance coherence is more
progressive familial Parkinson’s and dementia with
affected than local coherence in AD whereas the
pallido-ponto-nigral degeneration. EEG revealed
opposite occurs in MID. (Leuchter et al., 1992, Comi
abnormal findings early in the disease and diffuse
et al., 1998). Pucci et al. (1998) showed that EEG
slowing became more prominent as the diseases pro-
spectral parameters could discriminate between AD
gressed. Fogelson et al. (2003) found EEG response
and MID. Jeong et al. (2001) using nonlinear methods
with rivastigmine treatment in PD patients with
of analysing EEG, found differences between AD and
dementia. The changes were characterised by an
MID. Seal et al. (1998), using qEEG during odour
increase in faster frequencies and they concluded that
detection and during serial subtraction correctly clas-
this may indicate increased arousal or improvements
sified 95% and 91% of subjects with AD or MID,
in the cognitive status of the patients as a consequence
respectively. But using brain autopsy Muller et al.
(1997b) found few correlations between EEG and cer-
Crystal et al. (1990) reported a slowing of the pos-
ebrovascular pathology. So on balance, while EEG
terior background rhythm and often a frontally domi-
may might distinguish pure MID from pure AD this
nant burst pattern in neuropathologically diagnosed
can probably be done just as well clinically. Of
LBD cases. They suggested that EEGs could help to
course, most patients have mixed MID/AD.
differentiate AD from diffuse Lewy body disease. Briel et al. (1999) reported a greater slowing of the
EEG in LBD than in AD. However Londos et al. (2003) using EEG and rCBF and Barber et al.
The EEG in Pick’s Disease is often associated with a
(2000) using EEG suggested that these could not dis-
normal EEG (Stigsby et al., 1981). EEG coherence is
tinguish between AD and LBD. A small study by
also no different from normal controls but delta and
Calzetti et al. (2002) suggested that the FIRDA (Fron-
theta powers were significantly increased in AD com-
tal Intermittent Rhythmic Delta Activity) could dis-
pared to frontal lobe dementia subjects. (Forstl et al.,
tinguish AD and LBD patients and could improve
1996). A study by Yener et al. (1996) found that using
the diagnostic accuracy of LBD. Therefore the role
five qEEG measurements they could reach an accu-
of EEG in LBD and PRD is unclear. The EEG is only
racy of 84.6% to distinguish between FTD and AD
likely to predict response to treatment, if this was also
and 100% from controls. The most informative qEEG
useful for Alzheimer’s patients (see below).
variables for distinguishing FTD and AD were rela-tive power from the temporal region in beta-2 bandand from the parietal region in the theta, alpha andbeta-2 bands. A combination of qEEG and neuropsy-
chological testing was the best predictor of FTDaccording to Lindau et al. (2003). Chan et al.
A significant increase of coherence in qEEG in
(2004) reported no significant difference in EEG
patients with AIDS, with or without cognitive impair-
appearance between FTD patients and AD patients
ment, has been reported particularly in long distance
connections (Newton et al., 1994). Alpha rhythmchanges are the earliest non-specific signs of HIVbrain involvement. Elevation of alpha amplitude
was associated with change in the mental state. Anti-
The EEG is abnormal in HD with low voltage in about
retroviral medication suppresses this alpha elevation
40% (Scott et al., 1972). Streletz et al. (1990) found
supporting the usefulness of qEEG in monitoring
increased theta and decreased alpha activity in patients
the effect of the drugs on the CNS (Baldeweg and
with HD. However the EEG does not predict which
Gruzelier, 1997). Also the reduction of intrahemi-
family members will eventually develop HD, and
spheric alpha coherence correlates with the degree
would never approach the accuracy of gene testing.
of cognitive impairment. (Fletcher et al., 1997).
Copyright # 2005 John Wiley & Sons, Ltd.
Int J Geriatr Psychiatry 2005; 20: 1038–1045.
The MACS study (Nuwer et al., 1992) has reported
no difference in the incidence of EEG abnormalities
in seropositive subjects when compared with serone-
Cholinesterase inhibitors shift activity patterns of
gative controls. Parisi et al. (1989) reported that EEG
EEG towards normal (Agnoli et al., 1983). Jelic
abnormality might be a predictor of CNS involve-
et al. (1998b) studied the longitudinal changes of
ment. Again, however, the diagnostic and severity
qEEG during long term tacrine treatment of patients
indices of HIV dementia are not those of EEG abnorm-
with AD. They found slowing of fast EEG frequencies
alities—rather, in HIV they are immunological and
provided some evidence of early decline in treatment
effectiveness. Four studies (Alhainen et al., 1991,Alhainen and Riekkinen, 1993, Knott et al., 2000,Almkvist et al., 2001) found that qEEG profiles after
a single test dose of Tacrine, were good predictors ofresponse to Tacrine. Studies with Rivastigmine have
In contrast Creutzfeldt-Jakob disease is associatedwith ‘Periodic sharp wave complexes’ (PSWCs),
found similar predictive capacity of EEG. (Adler
which are highly characteristic of CJD (Levy et al.,
and Brassen, 2001, Brassen and Adler, 2003, Adleret al
1986). Steinhoff et al. (1996) found a specificity of
., 2004). Alpha and Delta frequencies in qEEG
86% and sensitivity of 67% in a blind EEG analysis
are also reduced by donepezil in AD (Reeves et al.
for PSWCs. PSWCs may exceptionally disappear in
2002; Balkan et al. 2003). In a longitudinal study of
the terminal stages of the disease (Aguglia et al.,
mild to mopderate AD patients, Rodriguez et al.
1997). Periodic sharp waves are usually generalised,
(2002) found that qEEG deterioration is reduced by
but they can be focal or lateralised (Cambier et al.,
Donepezil. Kogan et al. (2001) examined the long-
2003). Although PSWCs have also been reported in
term effect of donepezil on the qEEG of 12 AD
cases of severe post-anoxic encephalopathy, herpes
patients at different stages of their illness. Patients
encephalitis, AIDS dementia, lithium toxic encepha-
with mild AD showed reduced mean absolute theta
lopathy, Binswanger’s disease and severe AD (Rosen,
activity in frontal and temporo-parietal areas. Thosewith moderate/severe AD showed decreased mean
1996), these clinical situations can be distinguishedusing history or laboratory tests. Steinhoff et al.
absolute beta 1 activity particularly in the frontal
(1998) presented a pathophysiological hypothesis on
and occipital areas. A recent study by Onofrj et al.
the development of PSWCs based on the assumption
(2003) showed that donepezil had a better effect in
that the specific periodicity of PSWCs results from
patients with fluctuating cognition than those without.
still functional but greatly impaired subcortico-
They found that EEG could identify patients who
cortical circuits. This specific pattern of neuronal
fluctuate and therefore predict the response to the
degeneration may very rarely arise in other diseases
treatment. In Parkinson’s Related Dementia too,
independent of their aetiology so that EEG patterns
increased relative alpha activity has been seen with
appear identical. They suggest the use of clinical
rivastigmine treatment (Fogelson et al., 2003). These
signs, laboratory data and EEG to reach a diagnosis
studies (some of them were open label) suggest that
of CJD. On the contrary, a clinical diagnosis of CJD
EEG is altered as a result of therapy with Cholinester-
should be re-evaluated if repeated EEG recording fail
ase inhibitors, and might usefully predict response in
to show PSWCs. Hansen et al. (1998) investigated
EEG findings and the evolution of clinical signs. They
concluded that PSWCs usually mark the terminalstage of CJD. In early stages FIRDA-like EEG activ-
The EEG is a relatively simple and inexpensive non-
ities (Frontal Intermittent Rhythmic Delta Activity)
invasive diagnostic tool which has a high sensitivity
should be regarded as compatible with the diagnosis
for distinguishing organic brain disease from func-
and further EEGs requested to demonstrate PSWCs
tional. This in itself is an asset in so far as there is
in advanced stages of CJD. Van Everbroeck et al.
often diagnostic uncertainty in mid to late life when
(2004) using WHO diagnostic criteria observed EEGs
new psychiatric diagnoses occur in previously well
typical for CJD in 52% of the autopsies with ‘defined’
individuals. The identification of organic disease in
CJD a rate that was less than other previously
such circumstances could help to guide treatment.
reported. They found the PSWCs in 52% of the
Better secondary prevention of further disability by
CJD patients, in three of the AD patients, in one with
encouraging treatment of lipid, sugar and lifestyle
might result. Once an organic diagnosis is clearly
Copyright # 2005 John Wiley & Sons, Ltd.
Int J Geriatr Psychiatry 2005; 20: 1038–1045.
present, the EEG has limited ability to distinguish dif-
Bennys K, Rondouin G, Vergnes C, Touchon J. 2001. Diagnostic
value of quantitative EEG in Alzheimer’s disease. NeurophysiolClin 31: 153–160.
The EEG also has potential in other situations.
Berg L, Danziger WL, Storandt M, Coben LA, Gado M, et al. 1984.
Firstly, if it were shown that EEG properly predicted
Predictive features in mild senile dementia of the Alzheimer
response to cholinesterase inhibitors and that the
response could be measured using qEEG then there
Brassen S, Adler G. 2003. Short-term effects of acetylcholinester-
ase inhibitor treatment on EEG and memory performance in
is the potential for better targeting of expensive med-
Alzheimer patients: an open, controlled trial. Pharmacopsychiatry
ications. Secondly, some rare diagnoses can be iden-
tified by EEG. If more widespread use of EEGs
Brenner RP, Ulrich RF, Spiker DG, Sclabassi RJ, Reynolds CF, 3rd,
enabled better identification of CJD, then perhaps this
et al. 1986. Computerized EEG spectral analysis in elderly nor-
alone would justify change. Achieving this would
mal, demented and depressed subjects. Electroencephalogr ClinNeurophysiol 64: 483–492.
require cheap, local qEEG testing for a substantial
Brenner RP, Reynolds CF, 3rd, Ulrich RF. 1989. EEG findings in
proportion of people with dementia. Agreement on
depressive pseudodementia and dementia with secondary
the best qEEG parameters to use in such circum-
depression. Electroencephalogr Clin Neurophysiol 72: 298–
stances would enable redesign of EEG services away
Brenner RP. 1993. EEG and Dementia. In Electroencephalography:
from specialist technicians and centres to simple local
Basic Principles, Clinical Application, and Related Files, 3rd
qEEG. While we accept that such changes require
edn, Niedermeyer E, Lopes da Silva F (eds). Williams &
development and testing, we do think that it now
important to start studying more routine EEGs in psy-
Briel RC, McKeith IG, Barker WA, Hewitt Y, Perry RH, et al. 1999.
chiatric services for people in mid to late life.
EEG findings in dementia with Lewy bodies and Alzheimer’sdisease. J Neurol Neurosurg Psychiatry 66: 401–403.
Calzetti S, Bortone E, Negrotti A, Zinno L, Mancia D. 2002. Frontal
intermittent rhythmic delta activity (FIRDA) in patients withdementia with Lewy bodies: a diagnostic tool? Neurol Sci
Adler G, Brassen S. 2001. Short-term rivastigmine treatment
reduces EEG slow-wave power in Alzheimer patients. Neuropsy-
Cambier DM, Kantarci K, Worrell GA, Westmoreland BF, Aksamit
AJ. 2003. Lateralized and focal clinical, EEG, and FLAIR MRI
Adler G, Brassen S, Chwalek K, Dieter B, Teufel M. 2004. Predic-
abnormalities in Creutzfeldt-Jakob disease. Clin Neurophysiol
tion of treatment response to rivastigmine in Alzheimer’s demen-
tia. J Neurol Neurosurg Psychiatry 75: 292–294.
Chan D, Walters RJ, Sampson EL, Schott JM, Smith SJ, Rossor
Adler G, Brassen S, Jajcevic A. 2003. EEG coherence in Alzhei-
MN. 2004. EEG abnormalities in frontotemporal lobar degenera-
mer’s dementia. J Neural Transm 110: 1051–1058.
Agnoli A, Martucci N, Manna V, Conti L, Fioravanti M. 1983.
Chiaramonti R, Muscas GC, Paganini M, Muller TJ, Fallgatter AJ,
Effect of cholinergic and anticholinergic drugs on short-term
et al. 1997. Correlations of topographical EEG features with
memory in Alzheimer’s dementia: a neuropsychological and
clinical severity in mild and moderate dementia of Alzheimer
computerized electroencephalographic study. Clin Neurophar-
type. Neuropsychobiol 36: 153–158.
Claus JJ, Kwa VI, Teunisse S, Walstra GJ, van Gool WA, et al.
Aguglia U, Gambardella A, Le Piane E, Messina D, Farnarier G,
1998a. Slowing on quantitative spectral EEG is a marker for rate
et al. 1997. Disappearance of periodic sharp wave complexes
of subsequent cognitive and functional decline in early Alzhei-
in Creutzfeldt-Jakob disease. Neurophysiol Clin 27: 277–282.
mer disease. Alzheimer Dis Assoc Disord 12: 167–174.
Alhainen K, Partanen J, Reinikainen K, Laulumaa V, Soininen H,
Claus JJ, Ongerboer de Visser BW, Walstra GJ, Hijdra A, Verbeeten
B, Jr., van Gool WA. 1998b. Quantitative spectral electroence-
responders by a single dose pharmaco-EEG in patients with
phalography in predicting survival in patients with early Alzhei-
Alzheimer’s disease. Neurosci Lett 127: 113–116.
mer disease. Arch Neurol 55: 1105–1111.
Alhainen K, Riekkinen PJ, Sr. 1993. Discrimination of Alzheimer
Claus JJ, Strijers RL, Jonkman EJ, Ongerboer de Visser BW, Jonker
patients responding to cholinesterase inhibitor therapy. Acta
C, et al. 1999. The diagnostic value of electroencephalography in
mild senile Alzheimer’s disease. Clin Neurophysiol 110: 825–
Almkvist O, Jelic V, Amberla K, Hellstrom-Lindahl E, Meurling L,
Nordberg A. 2001. Responder characteristics to a single oral
Claus JJ, Ongerboer De Visser BW, Bour LJ, Walstra GJ, Hijdra A,
dose of cholinesterase inhibitor: a double-blind placebo-
et al. 2000. Determinants of quantitative spectral electroence-
controlled study with tacrine in Alzheimer patients. Dement
phalography in early Alzheimer’s disease: cognitive function,
regional cerebral blood flow, and computed tomography. Dement
Baldeweg T, Gruzelier JH. 1997. Alpha EEG activity and subcorti-
cal pathology in HIV infection. Int J Psychophysiol 26: 431–442.
Coben LA, Danziger W, Storandt M. 1985. A longitudinal EEG
Balkan S, Yaras N, Mihci E, Dora B, Agar A, Yargicoglu P. 2003.
study of mild senile dementia of Alzheimer type: changes at 1
Effect of donepezil on EEG spectral analysis in Alzheimer’s dis-
year and at 2.5 years. Electroencephalogr Clin Neurophysiol
ease. Acta Neurol Belg 103: 164–169.
Barber PA, Varma AR, Lloyd JJ, Haworth B, Snowden JS, Neary D.
Comi GC, Fornara C, Locatelli T, et al. 1998. EEG coherence in
2000. The electroencephalogram in dementia with Lewy bodies.
Alzheimer’s disease and multi-infarct dementia. Arch Gerontol
Copyright # 2005 John Wiley & Sons, Ltd.
Int J Geriatr Psychiatry 2005; 20: 1038–1045.
Crystal HA, Dickson DW, Lizardi JE, Davies P, Wolfson LI. 1990.
Jelic V, Johansson SE, Almkvist O, Shigeta M, Julin P, et al. 2000.
Antemortem diagnosis of diffuse Lewy body disease. Neurology
Quantitative electroencephalography in mild cognitive impair-
ment: longitudinal changes and possible prediction of Alzhei-
d’Onofrio F, Salvia S, Petretta V, Bonavita V, Rodriguez G,
mer’s disease. Neurobiol Aging 21: 533–540.
Tedeschi G. 1996. Quantified-EEG in normal aging and demen-
Jeong J, Chae JH, Kim SY, Han SH. 2001. Nonlinear dynamic ana-
tias. Acta Neurol Scand 93: 336–345.
lysis of the EEG in patients with Alzheimer’s disease and vascu-
Dunkin JJ, Osato S, Leuchter AF. 1995. Relationships between
lar dementia. J Clin Neurophysiol 18: 58–67.
EEG coherence and neuropsychological tests in dementia. Clin
Knott V, Mohr E, Mahoney C, Ilivitsky V. 2000. Pharmaco-EEG
test dose response predicts cholinesterase inhibitor treatment
Edwards-Lee T, Cook I, Fairbanks L, Leuchter A, Cummings JL.
outcome in Alzheimer’s disease. Methods Find Exp Clin Phar-
2000. Quantitative electroencephalographic correlates of psy-
chosis in Alzheimer disease. Neuropsychiatry Neuropsychol
Kogan EA, Korczyn AD, Virchovsky RG, Klimovizky S, Treves
TA, Neufeld MY. 2001. EEG changes during long-term treat-
Erkinjuntti T, Larsen T, Sulkava R, Ketonen L, Laaksonen R, Palo J.
ment with donepezil in Alzheimer’s disease patients. J Neural
1988. EEG in the differential diagnosis between Alzheimer’s dis-
ease and vascular dementia. Acta Neurol Scand 77: 36–43.
Kowalski JW, Gawel M, Pfeffer A, Barcikowska M. 2001. The
Fletcher DJ, Raz J, Fein G. 1997. Intra-hemispheric alpha coher-
diagnostic value of EEG in Alzheimer disease: correlation with
ence decreases with increasing cognitive impairment in HIV
the severity of mental impairment. J Clin Neurophysiol 18: 570–
patients. Electroencephalograp & Clin Neurophysiol 102: 286–
Lehtovirta M, Partanen J, Kononen M, Hiltunen J, Helisalmi S,
Fogelson N, Kogan E, Korczyn AD, Giladi N, Shabtai H, Neufeld
et al. 2000. A longitudinal quantitative EEG study of Alzhei-
MY. 2003. Effects of rivastigmine on the quantitative EEG in
mer’s disease: relation to apolipoprotein E polymorphism.
demented Parkinsonian patients. Acta Neurol Scand 107: 252–
Dement Geriatr Cogn Disord 11: 29–35.
Leocani L, Comi G. 1999. EEG coherence in pathological condi-
Forstl H, Besthorn C, Hentschel F, Geiger-Kabisch C, Sattel H,
tions. J Clin Neurophysiol 16: 548–555.
Schreiter-Gasser U. 1996. Frontal lobe degeneration and Alzhei-
Leuchter AF, Spar JE, Walter DO, Weiner H. 1987. Electroencepha-
mer’s disease: a controlled study on clinical findings, volumetric
lographic spectra and coherence in the diagnosis of Alzheimer’s-
brain changes and quantitative electroencephalography data.
type and multi-infarct dementia. A pilot study. Arch Gen Psy-
Hansen HC, Zschocke S, Sturenburg HJ, Kunze K. 1998. Clinical
Leuchter AF, Newton TF, Cook IA, Walter DO, Rosenberg-
changes and EEG patterns preceding the onset of periodic sharp
Thompson S, Lachenbruch PA. 1992. Changes in brain func-
wave complexes in Creutzfeldt-Jakob disease. Acta Neurol
tional connectivity in Alzheimer-type and multi-infarct demen-
Helkala EL, Laulumaa V, Soininen H, Partanen J, Riekkinen PJ.
Levy SR, Chiappa KH, Burke CJ, Young RR. 1986. Early evolution
1991. Different patterns of cognitive decline related to normal
and incidence of electroencephalographic abnormalities in
or deteriorating EEG in a 3-year follow-up study of patients with
Creutzfeldt-Jakob disease. J Clin Neurophysiol 3: 1–21.
Alzheimer’s disease. Neurology 41: 528–532.
Lindau M, Jelic V, Johansson SE, Andersen C, Wahlund LO,
Hughes J. 1995. The EEG in psychiatry: an outline with summar-
Almkvist O. 2003. Quantitative EEG abnormalities and cogni-
ized points and references. Clin Electroencephalograp 26: 92–
tive dysfunctions in frontotemporal dementia and Alzheimer’s
disease. Dement Geriatr Cogn Disord 15: 106–114.
Hughes JR. 1996. A review of the usefulness of the standard EEG in
Londos E, Passant U, Brun A, Rosen I, Risberg J, Gustafson L.
psychiatry. Clin Electroencephalograp 27: 35–39.
2003. Regional cerebral blood flow and EEG in clinically diag-
Hughes JR, John ER. 1999. Conventional and Quantitative Electro-
nosed dementia with Lewy bodies and Alzheimer’s disease. Arch
encephalography in Psychiatry. J Neuropsychiatry Clin Neurosci
Lopez OL, Brenner RP, Becker JT, Ulrich RF, Boller F, DeKosky
Ihl R, Brinkmeyer J, Janner M, Kerdar MS. 2000. A comparison of
ST. 1997. EEG spectral abnormalities and psychosis as predic-
ADAS and EEG in the discrimination of patients with dementia
tors of cognitive and functional decline in probable Alzheimer’s
of the Alzheimer type from healthy controls. Neuropsychobiol
Montplaisir J, Petit D, McNamara D, Gauthier S. 1996. Compari-
Jelic V, Shigeta M, Julin P, Almkvist O, Winblad B, Wahlund LO.
sons between SPECT and quantitative EEG measures of cortical
1996. Quantitative electroencephalography power and coherence
impairment in mild to moderate Alzheimer’s disease. Eur Neurol
in Alzheimer’s disease and mild cognitive impairment. Dementia
Moretti DV, Babiloni C, Binetti G, Cassetta E, Dal Forno G, et al.
Jelic V, Julin P, Shigeta M, Nordberg A, Lannfelt L, et al. 1997.
2004. Individual analysis of EEG frequency and band power in
Apolipoprotein E epsilon4 allele decreases functional connectiv-
mild Alzheimer’s disease. Clin Neurophysiol 115: 299–308.
ity in Alzheimer’s disease as measured by EEG coherence.
Muller TJ, Thome J, Chiaramonti R, Dierks T, Maurer K, et al.
J Neurol Neurosurg Psychiatry 63: 59–65.
1997a. A comparison of qEEG and HMPAO-SPECT in relation
Jelic V, Blomberg M, Dierks T, Basun H, Shigeta M, et al. 1998a.
to the clinical severity of Alzheimer’s disease. Eur Arch Psychia-
EEG slowing and cerebrospinal fluid tau levels in patients with
cognitive decline. Neuroreport 9: 157–160.
Muller HF, Engelsmann F, Nair NP, Robitaille Y. 1997b. Psychoger-
Jelic V, Dierks T, Amberla K, Almkvist O, Winblad B, Nordberg A.
iatric clinical, electro-encephalographic and autopsy findings.
1998b. Longitudinal changes in quantitative EEG during long-
term tacrine treatment of patients with Alzheimer’s disease. Neu-
Musha T, Asada T, Yamashita F, Kinoshita T, Chen Z, et al. 2002.
A new EEG method for estimating cortical neuronal impairment
Copyright # 2005 John Wiley & Sons, Ltd.
Int J Geriatr Psychiatry 2005; 20: 1038–1045.
that is sensitive to early stage Alzheimer’s disease. Clin Neuro-
during long-term donepezil therapy. Neuropsychobiology 46:
Newton TF, Leuchter AF, Walter DO, et al. 1994. Electroencepha-
Rosen I. 1996. Electroencephalography as a diagnostic tool in
lographic coherence in acquired immune deficiency syndrome.
dementia; a review. Acta Neurol Scand Suppl 168: 63–70.
Sato K, Kamiya S, Okawa M, Hozumi S, Hori H, Hishikawa Y.
Nobili F, Copello F, Vitali P, Prastaro T, Carozzo S, et al. 1999.
1996. On the EEG component waves of multi-infarct dementia
Timing of disease progression by quantitative EEG in Alzhei-
seniles. Int J Neurosci 86: 95–109.
mer’s patients. J Clin Neurophysiol 16: 566–573.
Seal ECJ, Van Hintum CJA, Pierson JM, Helme RD. 1998. Quanti-
Nuwer MR, Miller EN, Visscher BR, et al. 1992. Asymptomatic
tative electroencephalography, with serial subtraction and odour
HIV infection does not cause EEG abnormalities: results from
detection in the differentiation of Alzheimer’s disease and vascu-
the Multicenter AIDS Cohort Study (MACS) Neurology 42(6):
lar dementia Arch Gerontol Geriatri 27: 115–126.
Scott DF, Heathfield KW, Toone B, Margerison JH. 1972. The EEG
Onofrj M, Thomas A, Iacono D, Luciano AL, Di Iorio A. 2003. The
in Huntington’s chorea: a clinical and neuropahological study.
effects of a cholinesterase inhibitor are prominent in patients
J Neurol Neurosurg Psychiatry 35: 97–102.
with fluctuating cognition: a part 3 study of the main mechanism
Signorino M, Pucci E, Belardinelli N, Nolfe G, Angeleri F. 1995.
of cholinesterase inhibitors in dementia. Clin Neuropharmacol
EEG spectral analysis in vascular and Alzheimer dementia. Elec-
troencephalogr Clin Neurophysiol 94: 313–325.
Parisi A, Di Perri G, Strosselli M, Nappi G, Minoli L, Rondanelli
Stam CJ, van der Made Y, Pijnenburg YA, Scheltens P. 2003. EEG
EG. 1989. Usefulness of computerized electroencephalography
synchronization in mild cognitive impairment and Alzheimer’s
in diagnosing, staging and monitoring AIDS-dementia complex.
disease. Acta Neurol Scand 108: 90–96.
Steinhoff BJ, Racker S, Herrendorf G, Poser S, Grosche S, et al.
Penttila M, Partanen JV, Soininen H, Riekkinen PJ. 1985. Quanti-
1996. Accuracy and reliability of periodic sharp wave complexes
tative analysis of occipital EEG in different stages of Alzhei-
in Creutzfeldt-Jakob disease. Arch Neurol 53: 162–166.
mer’s disease. Electroencephalogr Clin Neurophysiol 60: 1–6.
Steinhoff BJ, Kropp S, Riedemann C, Eckardt KM, Herrendorf G,
Pijnenburg YA, van der Made Y, van Cappellen, et al. 2004. EEG
Poser S. 1998. [Elecroencephalographic charactistics of Creutz-
synchronization likelihood in mild cognitive impairment and
feldt-Jakob disease and its differential diagnosis]. Fortschr Neu-
Alzheimer’s disease during a working memory task. Clin Neuro-
Stigsby B, Johannesson G, Ingvar DH. 1981. Regional EEG
Pozzi D, Vazquez S, Petracchi M, Dancygier G, Garcia H,
analysis and regional cerebral blood flow in Alzheimer’s and
Starkstein S. 1996. Quantified electroencephalographic corre-
Pick’s diseases. Electroencephalogr Clin Neurophysiol 51:
lates of relative frontal or parietal hypoperfusion in dementia.
J Neuropsychiatry Clin Neurosci 8: 26–32.
Streletz LJ, Reyes PF, Zalewska M, Katz L, Fariello RG. 1990.
Prichep LS, John ER, Ferris SH, Reisberg B, Almas M, et al. 1994.
Computer analysis of EEG activity in dementia of the
Quantitative EEG correlates of cognitive deterioration in the
Alzheimer’s type and Huntington’s disease. Neurobiol Aging
elderly. Neurobiol Aging 15: 85–90.
Pucci E, Cacchio´ G, Angeloni R, et al. 1998. EEG spectral analysis
Strijers RL, Scheltens P, Jonkman EJ, de Rijke W, Hooijer C, Jonker
in Alzheimer’s disease and different degenerative dementias.
C. 1997. Diagnosing Alzheimer’s disease in community-dwell-
Arch Gerontol Geriatr 26: 283–297.
ing elderly: a comparison of EEG and MRI. Dement Geriatr
Pucci E, Belardinelli N, Cacchio G, Signorino M, Angeleri F. 1999.
EEG power spectrum differences in early and late onset forms of
Van Everbroeck B, Dobbeleir I, De Waele M, De Deyn P, Martin JJ,
Alzheimer’s disease. Clin Neurophysiol 110: 621–631.
Cras P. 2004 Differential diagnosis of 201 possible Creutzfeldt-
Reeves RR, Struve FA, Patrick G. 2002. The effects of donepezil on
Jakob disease patients. J Neurol 251(3): 298–304.
quantitative EEG in patients with Alzheimer’s disease. Clin
Weiner H, Schuster DB. 1956. The electroencephalogram in
dementia. Some preliminary observations and correlations. Elec-
Robinson DJ, Merskey H, Blume WT, Fry R, Williamson PC,
troencephalogr Clin Neurophysiol 8: 479–488.
Hachinski VC. 1994. Electroencephalography as an aid in the
Wszolek Z, Herkes GK, Lagerlund TD, Kokmen E. 1992. Compar-
exclusion of Alzheimer’s disease. Arch Neurol 51: 280–284.
ison of EEG background frequency analysis, psychologic test
Rodriguez G, Nobili F, Rocca G, De Carli F, Gianelli MV, Rosadini
scores, short test of mental status, and quantitative SPECT in
G. 1998. Quantitative electroencephalography and regional cer-
dementia. J Geriatr Psychiatry Neurol 5: 22–30.
ebral blood flow: discriminant analysis between Alzheimer’s
Wszolek ZK, Lagerlund TD, Steg RE, McManis PG. 1998. Clinical
patients and healthy controls. Dement Geriatr Cogn Disord 9:
neurophysiologic findings in patients with rapidly progressive
familial parkinsonism and dementia with pallido-ponto-nigral
Rodriguez G, Copello F, Vitali P, Perego G, Nobili F. 1999a. EEG
degeneration. Electroencephalogr Clin Neurophysiol 107: 213–
spectral profile to stage Alzheimer’s disease. Clin Neurophysiol
Yener GG, Leuchter AF, Jenden D, Read SL, Cummings JL, Miller
Rodriguez G, Nobili F, Copello F, Vitali P, Gianelli MV, et al.
BL. 1996. Quantitative EEG in frontotemporal dementia. Clin
1999b. 99mTc-HMPAO regional cerebral blood flow and quan-
titative electroencephalography in Alzheimer’s disease: a corre-
Yoshimura M, Isotani T, Yagyu T, Irisawa S, Yoshida T, et al. 2004.
lative study. J Nucl Med 40: 522–529.
Global approach to multichannel electroencephalogram analysis
Rodriguez G, Vitali P, De Leo C, De Carli F, Girtler N, Nobili F.
for diagnosis and clinical evaluation in mild Alzheimer’s disease.
2002. Quantitative EEG changes in Alzheimer patients
Copyright # 2005 John Wiley & Sons, Ltd.
Int J Geriatr Psychiatry 2005; 20: 1038–1045.
PREPARING FOR MISSION? Issues to consider if you are in mid life. Introduction This information is designed for second wind people who have already worked through some of the initial stages of reflection and prayer and have arrived at the place where they feel God has called them – either to seriously explore further, or maybe to go and check out an opportunity on the ground,
Elenco Atti Filtri impostati - atti adottati; tipo atto: Delibere di Giunta (GDG); con n. adozione dal: 118 al: 161 per l'anno: 2009 Attività Segreteria / Sedute Tipo Atto Proponente N. Adozione Data Iniz. Adozione Archiviazio Esecutività CENTRO CANOA ECANOTTAGGIO di San Giorgio diNogaro. Miglioramento funzionalealtri al servizio delle attività sportive. Approvazi
 nitively impaired individuals with elevated CSF tauprotein levels. Lehtovirta et al. (2000) found thatAD patients carrying the Apolipoprotein sigma4allele had more pronounced slow wave activity thanAD patients without the sigma4 allele. Examiningthe ApoE epsilon 4 allele, Jelic et al. (1997) foundthat ApoE epsilon4 allele does not influence EEGslowing but it was associated with a decrease in func-tional connectivity.
nitively impaired individuals with elevated CSF tauprotein levels. Lehtovirta et al. (2000) found thatAD patients carrying the Apolipoprotein sigma4allele had more pronounced slow wave activity thanAD patients without the sigma4 allele. Examiningthe ApoE epsilon 4 allele, Jelic et al. (1997) foundthat ApoE epsilon4 allele does not influence EEGslowing but it was associated with a decrease in func-tional connectivity.