Tadalafil entfaltet seine Wirkung über eine selektive Hemmung der PDE5, wodurch die Konzentration von cGMP im glatten Muskelgewebe stabil bleibt. Diese biochemische Modulation resultiert in einer langanhaltenden Relaxation der Gefäßwände. Der Wirkstoff wird nach oraler Einnahme effizient resorbiert, mit einer Bioverfügbarkeit von rund 80 %. Seine Halbwertszeit von bis zu 36 Stunden ist innerhalb dieser Substanzklasse außergewöhnlich. Abgebaut wird er in der Leber, hauptsächlich durch CYP3A4, mit anschließender biliärer Exkretion. Typische unerwünschte Wirkungen entstehen durch eine verstärkte Vasodilatation, etwa Kopfschmerzen oder Flush. Pharmakologisch wird cialis generika vor allem durch die verlängerte Wirkungsdauer charakterisiert.
The study of cardiac function during anesthesia by phonocardiogram
JOURNAL OF ELECTRONIC SCIENCE AND TECHNOLOGY OF CHINA, VOL. 6, NO. 1, MARCH 2008
Effect of Mixed Anesthesia on Cardiac Function by Phonocardiogram
Fei Han, Hong-Mei Yan, Xin-Chuan Wei, and Qing Yan
Abstract⎯Objective of this investigation is to further
testing are highly consistent and strongly suggestive of
analyze the cardiac function status change by phonocar-
changes in myocardial function, and they pointed out that
diogram during mixed anesthesia which is conducted by
heart sound changes during stress may be more rapid and
midazolam, skelaxin, fentanyi and propofol. The results
sensitive than changes in heart rate and blood pressure [2].
show that blood pressure, heart rate, amplitude of R wave
In recent years, Xiao S. Z. et al. sponsored that
and T wave, amplitude of first heart sound (S
phonocardiogram as a noninvasive, high benefit/cost ratio,
second heart sound (S
and portable method can be used for the evaluation of cardiac
2) about 37 subjects after anesthesia decrease compared with baseline, while the ratio of first
performance at the bedside and sports field, and so on [3],[4].
heart sound and second heart sound (S
They even proposed some new indicators to evaluate specific
1/S2) and the ratio of diastole duration and systole duration (D/S) increase.
cardiovascular status, such as the ratio of S1 amplitude to S2
Our study demonstrates that phonocardiogram as a
amplitude (S1/S2), which can be used to evaluate the
noninvasive, high benefit/cost ratio, objective, repeatable
dynamically changing relation between cardiac contractility
and portable method can be used for the monitoring and
and peripheral vascular pressure, including up-regulating
evaluation of cardiac function status during anesthesia
condition of cardiac contractility during stress; and the ratio
of diastolic to systolic duration (D/S), which can be used to
evaluate the time of blood flowing to the heart per se during
Index Terms⎯Anesthesia, cardiac function, phono- cardiogram.
Early studies reported that different anesthesia regimens
and anesthesia styles had different significant effects on
1. Introduction
cardiovascular function[6]. However, most of these studies were carried out by cardiac catheterization method or
In the course of anesthesia and operations, accurate,
echocardiography in animals[7]. There is a lack of one effect-
reliable, non-invasive and convenient measurement or moni-
tive, non-invasive, continuously monitoring and convenient
toring of cardiac function is critical for patients, especially
method to evaluate the patient’s cardiovascular function
for heart failure patients. At present, two methods are usually
during anesthesia and operations for above described reason.
used for cardiac evaluations in clinic. One is cardiac catheter-
Studies by Gerard R. et al. showed that heart sound
rization method, which is accurate and reliable, but invasive
characteristics can be used to monitor cardiac function
and not suitable for normal monitoring. The other is echo-
during halothane anesthesia in children, and the changes
cardiography, which is comparative expensive and inconve-
occur rapidly and precede noticeablely in heart rate and
blood pressure[8]. In their studies, they didn’t assess the
Hansen PB’s early animal researches showed that there
new indicators of cardiovascular status by heart sound and
was a very close relationship between the amplitude of the
halothane, what they used was a single inhaled anesthetic.
first heart sound (S1) and the cardiac contractility and
However, a mixed injected anesthesia of midazolam,
provided the possibility of phonocardiography as a monitor
skelaxin, fentanyi and propofol was another important
of cardiac performance during anesthesia [1]. Luisada A. A.
anesthetic style often used in clinic. Therefore, the object-
et al. suggested that heart sounds should be studied during
tive of this investigation was to further analyze the effect
anesthesia because the changes that occur during stress
of mixed anesthesia on cardiac function status change
Manuscript received July 10, 2007; revised October 12, 2007. This work
was supported by the National Nature Science Foundation of China under Grant No. 30400105, 973 Project under Grant No. 2003CB716106, and
2. Experiments
Outstanding Youth Fund of China under Grant No. 30525030.
2.1 Experimental Subjects
F. Han, H.-M. Yan, and Q. Yan are with School of Life Science and
Technology, University of Electronic Science and Technology of China, Chengdu
After approval of the Review Committee of Sichuan
610054 China (Corresponding author’s e-mail: hmyan@uestc.edu.cn).
University on research involving human subjects and
X.-C. Wei is with Department of Anesthesia Medical Center of Huaxi,
Sichuan University, Chengdu, 610064, China.
informed consent given by every subject was obtained, we
JOURNAL OF ELECTRONIC SCIENCE AND TECHNOLOGY OF CHINA, VOL. 6, NO. 1, MARCH 2008
carried out this study in Medical Center of Huaxi, Sichuan
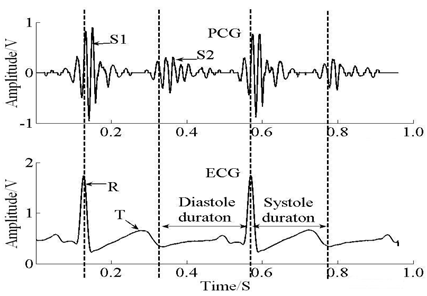
20~40 ms after R waves of ECG and S2 which is primarily
University, Chengdu, China. 37 ASA physical status I and II
decided by the closure pressure of the arotic and pulmonary
patients aged 18 years to 80 years presenting for urologic
occurs after the isovolumetric relaxation period during
surgery participated in the test. In clinic, midazolam, skelaxin,
diastole, before or after the end of T waves[12]. As
fentanyi and propofol, being as mixed anesthesia, was used
synchronous phase, it is proposed that the coordinate position
for patients, which dosages was determined by patients’
of R waves is regarded as the beginning of systole duration;
weight. Patients with serious cardiac disease or contraindi-
the coordinate location of the end of T waves is regarded as
cation to mixed anesthesia were excluded.
2.2 Experimental 3. Results
No preoperative medications were given, and all patients
had received nothing by mouth for at least 12 hours. In the
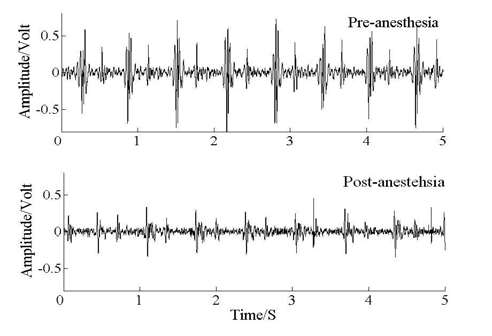
Characteristic heart sound waveforms before anesthesia
operating room, a metallic 3 cm diameter heart sound sensor
and after anesthesia are shown in Fig. 2. The amplitude of S1
with a flat frequency response between 35 Hz and 20000 Hz
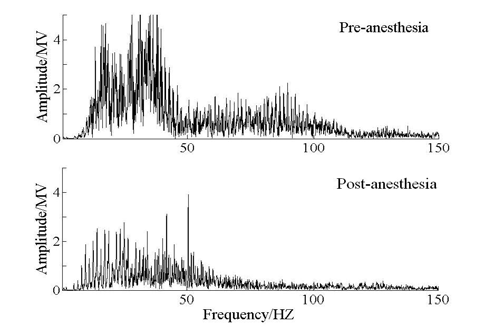
and S2 after anesthesia descends obviously. Fast Fourier
(BIOPAC Systems, Inc., USA) was placed at the position of
transform tracings for one patient before anesthesia and after
maximum S1 assisted by stethoscope; generally, it was
anesthesia are illustrated in Fig. 3. Likewise, the amplitude of
between the third and fourth rib[9]. The audio signals were
spectral edge after anesthesia drops obviously. These results
amplified and routed to a notebook PC (sampling rate are agreed with Gerard R’s early research [8]. 5000 Hz) and continuously monitored by Biopac MP150 (BIOPAC Systems, Inc., USA) from 2 minutes before
anesthesia to 2 minutes after anesthesia. The waveforms were
processed with Coifman fourth order wavelet basis to
minimize high-frequency noise and the resulting waveforms
were processed with Matlab 7.0 [10],[11].
The electrocardiograph (ECG) was monitored
synchronously with Biopac MP150; at the same time, blood
pressure and pulse oximeter et al. were monitored with anesthesia monitoring instruments (Shenzhen Mindray
Bio-medical electronics Co., LTD, China).
Fig. 2 Representative heart sound waveforms before anesthesia and
Fig. 1. The relationship of PCG and ECG.
Two representative audio samples were selected for each
patient: baseline (20 seconds), anesthesia duration (20
seconds, after anesthesia had been taking effect). The
variance of heart rate, blood pressure, amplitude of R wave
Fig. 3. Fast Fourier transform tracings for one patient before
and T wave, amplitude of S1 and S2, ratio of S1/S2 and D/S
from baseline to anesthesia duraiton were analyzed. The
results are presented as Mean ±Std. Thereinto, the systole and
Table 1 gives out the comparison of blood pressure, heart
diastole duration were located by classical method referred
rate and amplitude of R wave and T wave before anesthesia
with ECG and PCG. The relationship of PCG and ECG is
and after anesthesia. From table 1, the average heart rate of 37
subjects fell from 79±13 bpm before anesthesia to 69±10 bpm
closure pressure of the mitral and tricuspid valves occurs at
after anesthesia. Similarly, after anesthesia, the average
the end of the isometric contraction period during systole,
systole and diastole pressure dropped from 127±23 mmHg
HAN et al: Effect of Mixed Anesthesia on Cardiac Function by Phonocardiogram
and 80±14 mmHg to 84±23 mmHg and 51±14 mmHg,
4. Discussion
As well, the amplitude of patients’ ECG descended. As the
Mixed injected anesthesia of midazolam, skelaxin,
absolute amplitude of ECG may be different for different
fentanyi and propofol can restrain the circular system, inhibit
patient, we defined the value of R wave and T wave at
cardiac muscle, and decrease peripheral vascular resistance
pre-anesthesia as 1 for baseline. From Table 1, the average
obviously, especially midazolam and propofol[13]. Peripheral
relative amplitude of R wave and T wave after anesthesia
vascular resistance mainly takes effect on diastole pressure,
declined to 0.8978±0.1575 and 0.9411±0.0659, respectively.
when it reduced, the pressure of diastole and systole would also reduce, especially pressure of diastole would reduce more
Table 1: Comparison of blood pressure, heart rate and amplitude of R
obviously. Heart rate influence cardiac cycle directly, if it
wave and T wave before anesthesia and after anesthesia
slowed down, the duration of diastole and systole would
increase, and the pressure of diastole and systole would decrease indirectly, especially the pressure of diastole [14].
After the mixed injected anesthesia took effect, peripheral
vascular resistance decreased greatly and heart rate slowed
down in a certain extent, which both resulted in the falling of
pressure of systole and diastole directly, especially diastole
pressure. As a result, blood pressure decreased obviously after
* The value of R wave and T wave before anesthesia were defined as
Decreased diastole pressure made the driving pressure in
The patients’ cardiac function indicators at pre-anesthesia
closure of the aortic and pulmonary valves decrease, which
and post-anesthesia are shown in Table 2. Although previous
was primary contributor to S2, ultimately induced the decrease
animal experiments and invasive and non-invasive clinical
in amplitude of S2. Similarly, decreased systole pressure made
trails have shown that there was a very close relationship
the driving pressure in the closure of the mitral and tricuspid valves decrease, which was major contributor to S
between the amplitude of the first heart sound (S
induced the decrease in amplitude of S
cardiac contractility, the absolute value of S
not be used to evaluate cardiac contractility, as it is affected
by some factors, such as the thickness of the chest wall and
1 after anesthesia, thus the ratio of S1 amplitude and S2
amplitude rose. Therefore, S1/S2 can be used to reflect the
cardiac function level. Therefore, relative values are usually
dynamically changing relation between cardiac contractility
adopted. Here, we defined the status of pre-anesthesia as
and peripheral pressure during anesthesia.
baseline, represented with 1. The values after anesthesia are
Likely, the decrease in heart rate made diastole duration
relative ones which are the ratio of anesthesia data to
and systole duration lengthened, but diastole duration
lengthened greater than systole duration, which makes D/S
Table 2: Comparison of patients’ cardiac function indicators at
increased, so D/S can be used to evaluate the time of blood
5. Conclusion
Generally speaking, the decrease of heart rate, the rising
of D/S and S1/S2, in a certain extent, are helpful for patients
with healthy cardiac condition to get through anesthesia and
operation. Whereas, some patients with heart diseases like
brachycardiac and arrhythmia, and so on, the changes may be
a burden to heart. It needs disposal carefully in clinic.
*The value of cardiac function indicators before anesthesia were
From above, the results of cardiac indicators by
phonocardiogram are consisting with the relative principle of
From Table 2, after anesthesia, the average S
physiology and pharmacology. Our study demonstrated that
amplitude of 37 subjects fell to 0.9258±0.3869 and phonocardiogram as a noninvasive, high benefit/cost ratio, 0.7491±0.3805, respectively; CCCT (the increase of S1 with
objective, repeatable and portable method can be used for the
monitoring and evaluation of cardiac function status during
1 recorded at baseline) decreased 0.0742 averagely;
however, S1/S2 increased to 1.4670±0.7717. Although systolic duration almost unchanged, the diastole duration extended to
References
1.2734±0.2515, so that after anesthesia, D/S went up to 1.2260±0.2294.
[1] P. B. Hansen, A. A. Luisada, and D. J. Miletich, “Phono-
cardiography as a monitor of cardiac performance during
JOURNAL OF ELECTRONIC SCIENCE AND TECHNOLOGY OF CHINA, VOL. 6, NO. 1, MARCH 2008
anesthesia,” Anesth Analg., vol. 68, no. pp. 385-387, 1989.
[11] T. R. Reed, N. E. Reed, and P. Fritzson, “Heart sound analysis
[2] A. A. Luisada, A. Singhal, and V. Knighten, “New index of
for symptom detection and computer-aided diagnosis,”
cardiac contractility during stress testing with treadmill,” Acta. Simulation Modeling Practice and Theory, vol. 12,
Cardiol, vol. 41, no. 1, pp. 31-39, 1986.
[3] S.-Z. Xiao, J. Cheng, and X.-M. Guo, “Study on the
[12] L. Zhao, Q. Li, Q.-Y. Shao, X.-L. Zhu, and H.-J. Zhou,
Significance and method of heart sound recognition,”
“Studies on the comparison of normal and abnormal heart
Biomedical Engineering Foreign Medical Sciences, vol. 27,
sound signals,” Journal of Medical Signal Process and Medical Instrument, Medical and Physics, vol. 17, no. 3,
[4] S.-Z. Xiao, Z.-G. Wang, and D.-Y. Hu, “Studying cardiac
contractility change trend to evaluate cardiac reserve,” IEEE
[14] J.-Y. Jiang, Theory and Practice of Clinical Anesthesia, 1st ed.
Engineering in Medicine and Biology, vol. 21, no. 1, pp. 74-76,
Beijing: Tsinghua University Publishment, 2006, ch. 5,
[5] S.-Z. Xiao, X.-M. Guo, and G.-C. Liu, “Studying the
[15] T. Yao, J.-M Cao, X.-L. Fan, and D.-N. ZHU, Physiology, 1st
significance of cardiac contractility variability,” IEEE
ed. Beijing: People Publishment, 2005, ch. 5, pp. 177-179.
Engineering in Medicine and Biology, vol. 19, no. 3, pp. 81-83,
Fei Han was born in Anhui, China, in 1982. He graduated from
[6] C. Y. T. Hart, J. C. Burnett, and M. M. Redfield, “Effects of
School of Life Science and Technology, University of Electronic
avertin versus xylazine-ketamine anesthesia on cardiac
Science and Technology of China (UESTC) in 2005. He is now
function in normal mice,” Am J. Physiol,2001, vol. 281, no. 5,
pursing his master’s degree with School of Life Science and
Technology, UESTC. His research interests are primarily in the area
[7] A. A. Chaves, D. M. Weinstein, and J. A. Bauer,
of signal processing and database system.
“Non-invasive echocardiographic studies in mice influence of
Hong-Mei Yan was born in Chongqing, China, in 1974. She
anesthetic regimen,” Life Sciences, vol. 69, no. 2, pp. 213-222,
received Ph.D. degree from Chongqing University in 2003. She is
now an associate professor with School of Life Science and
[8] G. R. Manecke, M. A. Nemirov, A. A. Bicker, R. N. Adsumelli,
Technology, UESTC. Her research interests include medical signal
and P. J. Poppers, “The effect of halothane on the amplitude
Xin-Chuan Wei was born in 1968. He graduated from Huaxi
and frequency characteristics of heart sounds in children,”
University of China in 1992 and received M.S. degree from Sichuan
Anesth Analg, vol. 88, no. 2, pp. 263-267, 1999.
University in 1999. His research interests include anesthesiology
[9] M. L. Rice and D. J. Doyle, “Comparison of phono-
cardiographic monitoring location,” in Proc. IEEE EBMC’95 Qing Yan was born in Chongqing, China, in 1984. She CD-ROM, Toronto, pp. 12-14, 1995.
graduated from the School of Life Science and Technology, UESTC
[10] X.-D. Hu and X.-Z Yu, Heart Auscultation and Phono-
in 2006. She is now pursing her Master’s degree with the School of
cardiogram, 1st ed. Beijing: Public Sanitation Publishment,
Life Science and Technology, UESTC. Her research interests
1981, ch. 4, ch. 5 and ch. 6, pp. 32-72.
include medical signal processing and digital image process.
EK WEET! 07 Vlak 2 en 3 Snaaksie Onderwyseres: Wat is die kortste maand van die jaar? Leerder: Mei – dit het net drie letters. A Wie, wat, waar? i a Raad van Provinsies Ek kom van rots, en ek kan jou laat beweeg. Seychelle Petrol Die petrolprys styg met 81c per liter. B Klop die Kurrikulum Wat is die eerste drie woorde van die aanhef tot die gronA
Single-pass CO2-laser skin resurfacing in combination with cold air cooling. Efficacy and patient satisfaction of a prospective side-by- side study Christian Raulin, Hortensia Grema, Laserklinik Karlsruhe, Karlsruhe, Germany Word count: 1998 Correspondence address: Christian Raulin, M.D. Laserklinik Karlsruhe Kaiserstr. 104 Germany 76133 Karlsruhe www: Abstract: Ablative
 JOURNAL OF ELECTRONIC SCIENCE AND TECHNOLOGY OF CHINA, VOL. 6, NO. 1, MARCH 2008
carried out this study in Medical Center of Huaxi, Sichuan
20~40 ms after R waves of ECG and S2 which is primarily
University, Chengdu, China. 37 ASA physical status I and II
decided by the closure pressure of the arotic and pulmonary
patients aged 18 years to 80 years presenting for urologic
occurs after the isovolumetric relaxation period during
surgery participated in the test. In clinic, midazolam, skelaxin,
diastole, before or after the end of T waves[12]. As
fentanyi and propofol, being as mixed anesthesia, was used
synchronous phase, it is proposed that the coordinate position
for patients, which dosages was determined by patients’
of R waves is regarded as the beginning of systole duration;
weight. Patients with serious cardiac disease or contraindi-
the coordinate location of the end of T waves is regarded as
cation to mixed anesthesia were excluded.
2.2 Experimental
JOURNAL OF ELECTRONIC SCIENCE AND TECHNOLOGY OF CHINA, VOL. 6, NO. 1, MARCH 2008
carried out this study in Medical Center of Huaxi, Sichuan
20~40 ms after R waves of ECG and S2 which is primarily
University, Chengdu, China. 37 ASA physical status I and II
decided by the closure pressure of the arotic and pulmonary
patients aged 18 years to 80 years presenting for urologic
occurs after the isovolumetric relaxation period during
surgery participated in the test. In clinic, midazolam, skelaxin,
diastole, before or after the end of T waves[12]. As
fentanyi and propofol, being as mixed anesthesia, was used
synchronous phase, it is proposed that the coordinate position
for patients, which dosages was determined by patients’
of R waves is regarded as the beginning of systole duration;
weight. Patients with serious cardiac disease or contraindi-
the coordinate location of the end of T waves is regarded as
cation to mixed anesthesia were excluded.
2.2 Experimental