Tadalafil entfaltet seine Wirkung über eine selektive Hemmung der PDE5, wodurch die Konzentration von cGMP im glatten Muskelgewebe stabil bleibt. Diese biochemische Modulation resultiert in einer langanhaltenden Relaxation der Gefäßwände. Der Wirkstoff wird nach oraler Einnahme effizient resorbiert, mit einer Bioverfügbarkeit von rund 80 %. Seine Halbwertszeit von bis zu 36 Stunden ist innerhalb dieser Substanzklasse außergewöhnlich. Abgebaut wird er in der Leber, hauptsächlich durch CYP3A4, mit anschließender biliärer Exkretion. Typische unerwünschte Wirkungen entstehen durch eine verstärkte Vasodilatation, etwa Kopfschmerzen oder Flush. Pharmakologisch wird cialis generika vor allem durch die verlängerte Wirkungsdauer charakterisiert.
Treating hepatitis c in the prison population is costsaving
Treating Hepatitis C in the Prison Population
Jennifer A. Tan,1 Tom A. Joseph,2 and Sammy Saab1,2
The prevalence of chronic hepatitis C infection in U.S. prisons is 12% to 31%. Treatment of this substantial portion of the population has been subject to much controversy, both medically and legally. Studies have demonstrated that treatment of chronic hepatitis C with pegylated interferon (PEG IFN) and ribavirin is a cost-effective measure in the general population; however, no study has addressed whether the same is true of the prison popu- lation. The aim of this study was to determine the cost-effectiveness of hepatitis C treatment with PEG IFN and ribavirin in the U.S. prison population. Cost-effectiveness was deter- mined via a decision analysis model employing Markov simulation. The cohort of prisoners had a distribution of genotypes and stages of fibrosis in accordance with prior studies evaluating inmate populations. The probability of transitioning from one health state to another, reinfection rates, in-prison and out-of-prison mortality rates, sustained viral re- sponse rates, costs, and quality of life weights were also obtained from the literature. Sensi- tivity analysis was performed. In a strategy without a pretreatment liver biopsy, treatment was cost-effective for all ages and genotypes. This model was robust to rates of disease progression, mortality rates, reinfection rates, sustained viral response rates, and costs. In a strategy employing a pretreatment liver biopsy, treatment was also cost-saving for prisoners of all ages and genotypes with portal fibrosis, bridging fibrosis, or compensated cirrhosis. Treatment was not cost-effective in patients between the ages of 40 and 49 with no fibrosis and genotype 1. Conclusion: Treatment of chronic hepatitis C with PEG IFN and ribavirin in U.S. prisons results in both improved quality of life and savings in cost for almost all segments of the inmate population. If the decision to treat hepatitis C is based on pharmaco- economic measures, this significant proportion of infected individuals should not be denied access to therapy. (HEPATOLOGY 2008;48:1387-1395.)
Hepatitis C infection is an important public striking,approximately29%to43%ofthetotalnumber
health problem in the United States, with 1.3%
of persons infected with hepatitis C in the United States
of the population chronically infected with the
pass through a correctional system each year.3
virus. An even larger proportion of the U.S. prison pop-
As of midyear 2006, the U.S. prison system was con-
ulation is affected, where the prevalence of chronic infec-
tinuing to grow in size, housing 2,245,189 inmates per
tion ranges from 12% to 31%,1 likely a result of increased
year, or 497 per every 100,000 persons in the United
rates of injection drug use within this group. Even more
States.3 The average length of incarceration has been in-creasing as well, placing a greater burden on prison healthcare systems to address chronic medical conditions such as
Abbreviations: HCV, hepatitis C virus; ICER, incremental cost-effectiveness ra-
hepatitis C. With the predicted cost of medical expendi-
tio; PEG IFN, pegylated interferon; QALY, quality-adjusted life year; SVR, sus-
tures related to hepatitis C rising to as high as $10.7
From the Departments of 1Medicine and 2Surgery, University of California at
billion from 2010 to 2019,4 the U.S. prison health care
system could see an estimated 15% to 60% increase in its
Received March 14, 2008; accepted June 23, 2008.
budget in the coming years.5 Consequently, the cost-ef-
Address reprint requests to: Sammy Saab, M.D., M.P.H., Pfleger Liver Institute,200 UCLA Medical Plaza, Suite 214, Box 957302, Los Angeles, CA 90095.
fectiveness of hepatitis C treatment in prisons has been a
E-mail: SSaab@mednet.ucla.edu; fax: 310-206-4197.Copyright 2008 by the American Association for the Study of Liver Diseases.
Proponents of treatment in prisons argue that we have
Published online in Wiley InterScience (www.interscience.wiley.com). DOI 10.1002/hep.22509
an ethical duty to provide prisoners with the contempo-
Potential conflict of interest: Dr. Saab is on the speakers’ bureau of Roche,
rary best practices in medical care. They suggest that treat-
Schering-Plough, and Three Rivers Pharmaceuticals.
ment of hepatitis C could be seamlessly integrated into
existing programs that successfully manage tuberculosis,
“hepatitis C,” “treatment,” “cost-effectiveness,” “pris-
human immunodeficiency virus, and other transmittable
ons,” “pegylated-interferon and ribavirin,” “combination
diseases. Treatment could feasibly reduce the incidence of
therapy,” “jails,” and “inmates.”
new hepatitis C virus (HCV) infections and prevent fu-
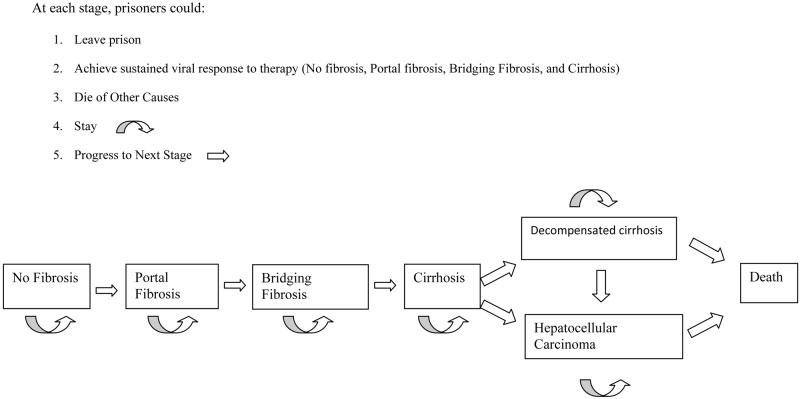
Using data obtained from these articles, we used the
ture complications from liver disease. Substance abuse
software Treeage Pro Health Module (Williamstown,
and risk reduction counseling could be employed simul-
MA) to construct a decision analysis model employing
taneously, resulting in enduring benefits outside of pris-
Markov simulation (Fig. 1). This allowed us to estimate
the incremental cost-effectiveness ratio (ICER) of combi-
Those who oppose treatment note that therapy is often
nation therapy for hepatitis C in the U.S. prison popula-
interrupted by prison release or transfer, and that contin-
tion and thus compare the strategy of treatment to that of
ued care for hepatitis C after release is often unavailable to
no treatment. The perspective adopted was that of the
what is a largely uninsured population. This could pro-
U.S. prison health care system. We used the generally
mote resistance to therapy or inadequate management of
accepted cost-effectiveness threshold of $50,000 per qual-
treatment-related adverse events. Furthermore, high rates
ity-adjusted life years (QALYs) as the maximum value for
of relapse to injection drug use or other high-risk activity
determining the preferred treatment option.
result in considerable rates of reinfection after prison re-
The target population at the beginning of our anal-
lease, which could be expected to undermine the benefits
ysis was a cohort of men, ages 40 to 49 years, who were
incarcerated in the U.S. prison system and chronically
Prior studies have demonstrated that treatment of
infected with hepatitis C as evidenced by positive sero-
chronic hepatitis C with pegylated interferon (PEG IFN)
logic tests and quantitative assays for HCV RNA. Their
and ribavirin is a cost-effective measure in the general
baseline demographics were assumed to be similar to
population.10-23 However, no study has yet addressed
that of the general U.S. prison population. In a bulletin
whether combination therapy would be cost-effective in
published by the Bureau of Justice in May 2006,24
the prison population. This study aims to answer this
Caucasians comprised the largest proportion of prison-
question in the male prison population, which makes up
ers at 44.3%, followed by African Americans at 38.9%
and Latinos at 15%. Men were 7 times more likely tobe imprisoned than females, and comprised 87.3% of
Patients and Methods
the prison population.24 The average age of the prison-
We conducted a MEDLINE search of the published
ers was 41 Ϯ 7 years.25 These demographics were con-
literature using various combinations of the search terms
sistent with the inmate populations studied in the
Table 1. Clinical Assumptions
-␣2b and ribavirin.29,30 Patients with all disease states ex-
Variable Baseline References
cept for decompensated cirrhosis and hepatocellular car-cinoma were eligible for treatment. Treatment was
administered for a total of 48 weeks in patients with ge-
notype 1 and for a total of 24 weeks in patients with
genotypes 2 and 3. We assumed that treatment was dis-
continued after 12 weeks in patients with genotype 1 who
did not achieve an early virologic response, defined as a
2-log reduction in their levels of HCV RNA.29 Antide-
pressants and growth factors such as erythropoeitin were
not used. Sustained viral response (SVR) rates were ob-
tained from the literature and were presumed to be iden-
tical to that of the general population— 42% for genotype
1 and 79% for genotypes 2 and 3.31-33 Although adher-
ence would likely approach 100%, given that medication
would be administered under the direct supervision of
prison health care officials, we nevertheless varied compli-
ance rates to account for patients who might discontinue
In all models, the prisoners transitioned in 6 month
Data are expressed as rates per year.
intervals through a variety of health states until death. Anaverage life expectancy of 75 years was used, as per the
published literature we used to make baseline assump-
average life expectancy of males in the United States.34
The probability of progression from one health state to
We presumed that genotype determination was per-
another was estimated from published literature looking
formed in all prisoners prior to commencement of ther-
at the natural history of HCV infection, and assumed to
apy. The inmates were accorded a distribution of
be equivalent for patients both inside and outside prison
genotypes as reported in the literature specific to the
(Table 2). In addition, prisoners could be released from
prison population: 78% were assumed to have genotype
prison or remain incarcerated at each stage of the model.
1, and 22% were assumed to have genotypes 2 and 3
They could be reinfected with HCV at a rate determined
Two strategies were then analyzed. In the first strategy,
Table 2. Transition Probabilities
prisoners did not undergo a liver biopsy prior to starting
Variable Baseline
treatment. They were assumed to have a distribution of
stages of fibrosis in accordance with the literature. Sterling
et al.25 conducted a retrospective study of 302 inmates in
Virginia with chronic hepatitis C who had undergone
liver biopsy and found that 30% of prisoners had no
fibrosis, 45% had portal fibrosis, 18% had bridging fibro-
sis, and 6% had cirrhosis (Table 1). An ICER was then
calculated for these prisoners as a pooled population in
In the second strategy, all prisoners underwent a liver
biopsy prior to beginning therapy in order to determine
their stage of fibrosis. A modified METAVIR scoring sys-
tem was used, and the patients were divided into four
groups: (1) no fibrosis, (2) portal fibrosis, (3) bridging
fibrosis, and (4) compensated cirrhosis.27,28 The most
cost-effective option was calculated for each group depen-
Treatment was assumed to follow current guidelines,
Data are expresses as rates per year and were obtained from references 10, 11,
using a combination of weight-based PEG IFN-␣2a or
Table 3. Costs Per Year
mum value the model would allow. Costs were halved and
Variable Baseline Reference
doubled to obtain lower and upper limits, and the annualdiscount rate ranged from 0% to 10%.
Our model found that treatment was cost-effective in
prisoners of all age ranges and genotypes when liver bi-
opsy was not a prerequisite to starting antiviral therapy
(first strategy). In other words, treatment resulted in both
Costs have been adjusted to 2007 U.S. dollars.
decreased costs and improved quality of life. In prisoners
*Costs consisted of clinic visits, laboratory tests, and adverse events.
between 40 and 49 years of age, treatment saved $41,321
†A composite cost was used for decompensated cirrhosis, taking into account
and increased QALYs by 0.75. For prisoners between 50
costs related to ascites, variceal bleeding, and hepatic encephalopathy.
and 59 years of age, treatment decreased costs by $33,445and increased QALYs by 0.69. In prisoners between 60
from prior studies, and they could die either from liver
and 69 years of age, treatment produced $11,637 in sav-
disease or other causes. Both reinfection rates and mortal-
ings and a gain of 0.5 in QALYs (Table 4). Sensitivity
ity rates were different in prison and out of prison (Table
analysis revealed that the model using this strategy was
1). It was assumed that mortality from liver disease could
robust to all variables, including in-prison and out-of-
only occur in patients with decompensated cirrhosis or
prison mortality rates, rates of disease progression, in-
hepatocellular carcinoma, and that mortality rates from
prison and out-of-prison reinfection rates, SVR rates, and
both liver and nonliver causes were similar across age
groups. Furthermore, we presumed that disease progres-
Treatment was also cost-effective for most situations
sion could still occur in patients with compensated cirrho-
employing pretreatment liver biopsy (second strategy). In
our base case population with portal fibrosis, treatment
Costs used in our analysis were obtained from the
resulted in $18,516 in saved costs and an increase in
literature and were adjusted to 2007 U.S. dollars (Ta-
QALYs of 0.58 (Table 5). It was also cost-effective in the
ble 3). We assumed that the absolute and incremental
base case populations with bridging fibrosis and compen-
costs of reinfection were identical to those incurred
sated cirrhosis. In prisoners with portal fibrosis and bridg-
with primary infection. Quality of life weights were
ing fibrosis, the model was sensitive to life expectancy,
similarly obtained and were assumed to be similar to
with treatment no longer cost-effective if lifespan after the
that of the general U.S. population. A discount rate of
initiation of therapy was less than 10 years. For these
populations, the model was robust to all other clinical
Sensitivity analysis was performed in order to address
our dynamic health care and economic system. Clinical
In the subset of patients who had no fibrosis on pre-
variables, costs, quality of life weights, and discount rate
treatment liver biopsy, treatment was not cost-effective in
were varied over wide ranges to assess their impact on the
those between ages 40-49 who had genotype 1, incurring
calculated ICERs. The ranges used for the clinical vari-
$3,367 in increased costs and a decrease in QALYs of 0.01
ables were based on data from the literature or, in cases
(Table 5). For patients in the same age group with geno-
where data was limited, were set from zero to the maxi-
types 2 or 3, however, treatment resulted in $10,844 in
Table 4. Summary of Costs, Efficacy, and ICERs for Strategy 1 (No Pretreatment Liver Biopsy) Efficacy (QALY) Treatment No Treatment Treatment No Treatment ICER, U.S. $ Table 5. Summary of Costs, Efficacy, and ICERs for Strategy 2 (Pretreatment Liver Biopsy) Efficacy (QALY) Treatment No Treatment Treatment No Treatment ICER, US $ No fibrosis Men, age 40–49 Portal fibrosis Bridging fibrosis Men, age 40–49 Compensated cirrhosis Men, age 40–49
saved costs and a gain in QALYs of 0.11. For this cohort,
Discussion
the model was sensitive to in-prison reinfection rates andnonliver mortality rates, with treatment no longer pre-
Our results demonstrate that PEG IFN and ribavirin
ferred if these rates increased to more than twice their
combination therapy is cost-effective in the prison popu-
baseline values. Cost-effectiveness was also affected by
lation, both in strategies with and without biopsy. Incor-
SVR rate, with a rate of less than 72.6% resulting in no
porating a pretreatment liver biopsy may be the most
treatment being favored, and by costs, with sums greater
cost-effective approach, however, as one could potentially
than $15,712 (baseline value $14,680) making treatment
exclude certain patients with no fibrosis from therapy.
Although we had not expected treatment to be cost-effec-
Treatment was cost-effective in patients with no fibro-
tive because of the high reinfection rates and nonliver
sis between 50 and 59 years of age and cost-effective but
mortality rates both inside and outside prison, treatment
not dominant in patients between 60 and 69 years of age,
remained cost-effective despite varying these factors over
with an ICER of $6,813/QALY (Table 5). The model was
robust to all variables for patients in these age groups with
The only segment of the prison population in which
treatment was not cost-effective was incarcerated individ-
uals between the ages of 40 and 49 with genotype 1 and
study comparing response rates to standard interferon be-
no fibrosis. Given their age and lack of liver damage, they
tween African Americans and Caucasians in the Virginia
have a lower probability than other groups of developing
correctional system found no significant difference in
cirrhosis and hepatic decompensation. Their disease pro-
SVR between the two groups, perhaps a result of increased
cess is largely silent, their quality of life is relatively unaf-
compliance with directly observed therapy.53 Further-
fected, and they are more likely to die from non–liver-
more, our model was robust to SVR rates varied over wide
related causes. SVR rates are low, and the benefits of
ranges in all cohorts except prisoners between 40-49 years
treatment are outweighed by the costs and morbidity of
of age with no fibrosis. Therefore, even if SVR was as low
treatment. On the other hand, although the risk of devel-
as 28% in African American inmates,52 treatment would
oping liver-related complications remains small in simi-
still be at least cost-effective for almost all prison cohorts.
larly aged patients with genotypes 2 and 3, higher SVR
Similarly, rates of fibrosis and disease progression in
rates make treatment more likely to result in benefits that
prisoners were assumed to be comparable to those of non-
outweigh other factors. The ICER for this group with no
prisoners. Although there are no studies evaluating
fibrosis between 40 and 49 years of age was particularly
whether the natural history of hepatitis C is identical in
sensitive to rates of SVR and costs of treatment, empha-
this population, we accounted for possible differences by
sizing that treatment in these patients is only worthwhile
varying rates of fibrosis and disease progression over wide
if it is highly effective or relatively inexpensive.
ranges. Because our model was robust to these variations,
Our study results apply only to prisoners in the United
this assumption is unlikely to be a source of bias.
States and are not meant to be applicable to the general
Costs and quality of life weights were also obtained
population. Nevertheless, prior cost-effective analyses
from studies of nonprison populations.39,49-51 Despite the
performed on nonprison cohorts show results similar to
increasing use of growth factors and antidepressants as
ours, with most studies demonstrating that treatment
adjuncts to treatment, we elected not to include these as
with PEG IFN and ribavirin is a cost-effective measure
potential costs. This is consistent with prior cost-effective
regardless of stage of fibrosis.10-23 Although our analysis
analyses of hepatitis C treatment in the general popula-
differed from that of Salomon et al.,10 who reported that
tion.10-23 Most pivotal trials of hepatitis C treatment,
treatment of men with no fibrosis was cost-effective in
from which we estimated the SVRs for our model, did not
patients with genotype 1 as well as patients with geno-
allow for growth factors, and their use may not be consis-
types 2 and 3, the Salomon et al. study compared treat-
tently available at all prison settings.31-33
ment with PEG IFN and ribavirin to treatment with
Although the incidence of depression during hepatitis
standard interferon and ribavirin, while our analysis com-
C treatment is not trivial (20%–30%),54 this additional
pared treatment based on PEG IFN with no treatment.
cost would be unlikely to impact our analysis, because it
Comparison to no treatment results in a substantially
remains small relative to the total cost of therapy. The
greater incremental difference in cost, which likely ac-
average wholesale cost of 12 months of the antidepressant
oral medication citalopram, for instance,54 is approxi-
This study is in large part limited by its reliance on data
mately $972.48 Assuming that 30% of the inmates would
obtained from prior literature rather than data gathered
require citalopram during treatment, this would represent
prospectively. The natural history of hepatitis C and its
less than 2% of the total cost of therapy.
response to treatment has not been studied extensively in
Moreover, the high background rate of depression in
the prison population, and we assumed for many aspects
the prison population (an estimated 23.5% in state pris-
of our model that the prison population would behave
ons and 16% in federal prisons)56 makes it difficult to
similarly to the general U.S. population.
distinguish which patients would require antidepressants
One such variable was rates of SVR, because only lim-
as a complication of therapy and which patients would
ited data exist on treatment response in prisoners. For
already require antidepressants regardless of antiviral ther-
instance, one published study assessed the efficacy of stan-
apy. In contrast, the baseline rate of depression in registry
dard rather than PEG IFN in prisoners in Rhode Island
trials was 1% to 5%32 and in the general U.S. population
but did not stratify outcomes according to genotype.26
is reported to be approximately 10.6%.56 Potential treat-
One might expect SVR rates to be lower in the prison
ment candidates in the prison setting would also need to
population, because prior studies have shown SVR rates
be carefully screened for other mental illnesses, because
to be significantly lower in African Americans than in
they can be found in up to 50% of state and federal
non–African Americans,52 and this group comprises a
larger proportion of the inmate population than the pop-
Although quality of life in prisoners is lower than that
ulations studied in registry trials. However, a retrospective
of the general population, hepatitis C infection has not
been shown to make a significant impact.57 This is likely
provided that they do not have contraindications such as
because non-HCV factors override HCV-specific quality
severe psychiatric or medical illness. Prisoners must also
of life impairment. Furthermore, nonviral HCV-specific
demonstrate a commitment to abstinence from alcohol
quality of life impairments are likely to be equally distrib-
and other substances. Genotyping is suggested for all pa-
uted between prisoners who are and who are not treated
tients, and liver biopsy is suggested for patients with ele-
vated alanine aminotransferase levels, genotype 1, or
Another assumption made in our model was that pa-
suspected compensated cirrhosis. The Bureau recom-
tients with cirrhosis who achieved SVR could still develop
mends that treatment not be initiated in short-term in-
decompensated cirrhosis and hepatocellular carcinoma at
mates, given the high likelihood that therapy will not be
rates similar to those who did not achieve SVR. This is a
completed.39 Enforcement of such a national guideline is
bias against treatment. Recent studies have demonstrated
problematic, however, because there is currently no cen-
that cirrhotic patients who have achieved SVR actually
trally funded or administered program to employ hepati-
have lower rates of hepatic decompensation and hepato-
tis C treatment. Each state manages its own budget and
cellular carcinoma than those who do not achieve
therefore adopts its own set of treatment guidelines.
Ethical considerations also play a large role in this mat-
Finally, the cohort we used for our model consisted of
ter of public controversy, and the cost-effectiveness of
only male prisoners. We felt this nevertheless resulted in
treatment must be weighed against these other concerns.
an adequate representation of the prison population, be-
As with liver transplantation, proponents of treatment
cause men are 7 times more likely to be imprisoned than
argue that it is unconstitutional to deny inmates access to
females and make up 87.3% of the U.S. prison popula-
treatment that is considered standard care. In 2003, Or-
tion.7 Furthermore, there have been no studies published
egon inmates filed a class-action lawsuit against the state
in the literature thus far showing significant sex differ-
prison system, alleging cruel and unusual punishment,
ences in regard to both the natural history of hepatitis C
and sought $17.5 million in medical expenses, drug ther-
infection or response rates to treatment.
apy, and potential liver transplantations (Anstett et al. v.
Currently, we are not aware of a standard policy on the
State of Oregon). A settlement was reached in 2004, re-
treatment of U.S. prisoners with chronic hepatitis C.
sulting in liberalization of the state’s hepatitis C treatment
Even screening for hepatitis C infection remains contro-
guidelines,59,60 and was considered by many to be a vic-
versial and is not universally performed.9 As of 2000,
1,209 of 1,584 state public and private adult correctional
Those who oppose therapy for prisoners, however,
facilities, housing 94% of all state prisoners, reported that
maintain that incarcerated individuals, by virtue of
they tested inmates for hepatitis C; 1,104 (70%) statecorrectional facilities reported that they had some type of
their offenses, have forfeited their right to receive these
policy for treating hepatitis C in their inmates. Between
resources,40 particularly as treatment would be admin-
July 1, 1999, and June 30, 2000, 4,750 inmates were
istered at the expense of taxpayers, while a large pro-
portion of uninsured patients continue to be denied
Policies vary widely from state to state, however. In
some states, written protocols exist for the treatment of
If the decision to treat is based on pharmaco-economic
prisoners, and in others, selection for treatment is per-
measures, however, the results of our analysis suggest that
formed on a case-by-case basis. In certain states, liver bi-
treatment is cost-saving and should not be withheld in
opsy is mandatory prior to treatment, and in others, the
U.S. prisoners with hepatitis C. Because the efficacy of
decision to biopsy is left to health care providers. A min-
treatment is diminished by relapse of injection drug use
imum prison sentence of 15 to 18 months is required by
and reinfection, this treatment strategy must be coupled
many states in order to assure completion of treatment
with educational and substance abuse programs. Further-
and adequate follow-up prior to release. A minority of
more, because mental illness is widespread in the prison
states do not have any established programs for hepatitis
population and can often be exacerbated by treatment,
careful mental health screening and follow-up would be
In order to address this issue, the Federal Bureau of
Prisons put forth a set of clinical practice guidelines in
In conclusion, although the ethical debate regarding
2005. They recommend that treatment be continued in
the implementation of treatment for hepatitis C in pris-
prisoners who are already on therapy and that therapy be
ons is not likely to be settled soon, we can assert that from
initiated in prisoners who meet criteria published by the
a pharmaco-economic standpoint, treatment of hepatitis
American Association for the Study of Liver Diseases,
C in the prison population is cost-effective. References
21. Lin WA, Tarn YH, Tang SL. Cost-utility analysis of different peg-inter-
feron alpha-2b plus ribavirin treatment strategies as initial therapy for naı¨ve
1. Spaulding AC, Weinbaum CM, Lau DT, Sterling R, Seeff LB, Margolis
Chinese patients with chronic hepatitis C. Aliment Pharmacol Ther 2006;
HS, et al. A framework for management of hepatitis C in prisons. Ann
22. Yeh WS, Armstrong EP, Skrepnek GH, Malone DC. Peginterferon alfa-2a
2. Hammett TM, Harmon MP, Rhodes W. The burden of infectious disease
versus peginterferon alfa-2b as initial treatment of hepatitis C virus infec-
among inmates of and releasees from US correctional facilities, 1997. Am J
tion: a cost-utility analysis from the perspective of the Veterans Affairs
Health Care System. Pharmacotherapy 2007;27:813-824.
3. U.S. Department of Justice. Prison and jail inmates at midyear 2006.
23. Grieve R, Roberts J, Wright M, Sweeting M, DeAngelis D, Rosenberg W,
Bureau of Justice Statistics Bulletin, June 2007. Available at: http://www.oj-
et al. Cost-effectiveness of interferon-alpha or peg-interferon alpha with
p.usdoj.gov/bjs/abstract/pjim06.htm. Accessed July 2008.
ribavirin for histologically mild chronic hepatitis C. Gut 2006;55:1332-
4. Wong JB, McQuillan GM, McHutchison JG, Poynard T. Estimating
future hepatitis C morbidity, mortality, and costs in the United States.
24. U.S. Department of Justice. Prison and jail inmates at midyear 2005.
Am J Public Health 2000;90:1562-1569. Bureau of Justice Statistics Bulletin, May 2006. Available at: http://www.oj-
5. Centers for Disease Control and Prevention. Prevention and control of
p.usdoj.gov/bjs/abstract/pjim05.htm. Accessed July 2008.
infections with hepatitis viruses in correctional settings. MMWR Morb
25. Sterling RK, Brown RS, Hofmann CM, Luketic VA, Stravits RT, Sanyal
AJ, et al. The spectrum of chronic hepatitis C virus infection in the Virginia
6. Weinbaum CM, Sabin KM, Santibanez SS. Hepatitis B, hepatitis C, and
Correctional System: development of a strategy for the evaluation and
HIV in correctional populations: a review of epidemiology and prevention.
treatment of inmates with HCV. Am J Gastroenterol 2005;100:313-321.
26. Allen SA, Spaulding AC, Osei AM, Taylor LE, Cabral AM, Rich JD.
7. Fox RK, Currie SL, Evans J, Wright TL, Tobler L, Phelps B, et al. Hepa-
Treatment of chronic hepatitis C in a state correctional facility. Ann Intern
titis C virus infection among prisoners in the California State Correctional
System. Clin Infect Dis 2005;41:177-186.
27. Scheuer PJ. Classification of chronic viral hepatitis: a need for reassess-
8. Hammett TM. Adopting more systematic approaches to hepatitis C treat-
ment in correctional facilities. Ann Intern Med 2003;138:235-236.
28. Desmet VJ, Gerber M, Hoofnagle JH, Manns M, Scheuer PJ. Classifica-
9. Spaulding A, Greene C, Davidson K, Schneidermann M, Rich J. Hepatitis
tion of chronic hepatitis: diagnosis, grading and staging. HEPATOLOGY
C in state correctional facilities. Prev Med 1999;28:92-100.
10. Salomon JA, Weinstein MC, Hammitt JK, Goldie SJ. Cost-effectiveness of
29. Kim AI, Saab S. Treatment of hepatitis C. Am J Med 2005;118:808-815.
treatment for chronic hepatitis C infection in an evolving patient popula-
30. Strader DB, Wright T, Thomas DL, Seeff LB. Diagnosis, management,
and treatment of hepatitis C. HEPATOLOGY 2004;39:1147-1171.
11. Siebert U, Sroczynski G, Rossol S, Wasem J, Ravens-Sieberer U, Kurth
31. Manns MP, McHutchinson JG, Gordon SC, Rustgi VK, Shiffman M,
BM, et al. Cost effectiveness of peginterferon ␣-2b plus ribavirin for initial
Reindollar R, et al, and the International Hepatitis Interventional Therapy
treatment of chronic hepatitis C. Gut 2003;52:425-432.
Group. Peginterferon alfa-2b plus ribavirin compared with interferon
12. Gerkens S, Nechelput M, Annemans L, Peraux B, Mouchart M, Beguin C,
alfa-2b plus ribavirin for initial treatment of chronic hepatitis C: a random-
et al. A health economic model to assess the cost-effectiveness of PEG IFN
ized trial. Lancet 2001;358;958-965.
␣-2a and ribavirin in patients with mild chronic hepatitis C. J Viral Hepat
32. Fried MW, Shiffman ML, Reddy R, Smith C, Marinos G, Goncales FL, et
al. Peginterferon alfa-2a plus ribavirin for chronic hepatitis C virus infec-
13. Lidgren M, Hollander A, Weiland O, Jo¨nsson B. Productivity improve-
tion. N Engl J Med 2002;347;975-982.
ments in hepatitis C treatment: impact on efficacy, cost, cost-effectiveness
33. Hadziyannis SJ, Sette H, Morgan TR, Balan V, Diago M, Marcellin P, et
and quality of life. Scand J Gastroenterol 2007;42:867-877.
al. Peginterferon-␣2a and ribavirin combination therapy in chronic hepa-
14. Bernfort L, Sennfalt K, Reichard O. Cost-effectiveness of peginterferon
titis C. Ann Intern Med 2004;140:346-355.
alfa-2b in combination with ribavirin as initial treatment for chronic hep-
34. Centers for Disease Control. United States life tables, 2003. National Vital
atitis C in Sweden. Scand J Infect Dis 2006;38:497-505. Statistics Reports, April 2006. Available at: http://www.cdc.gov/nchs/prod-
15. Buti M, Medina M, Casado MA, Wong JB, Fosbrook L, Esteban R. A
ucts/pubs/pubd/lftbls/life/1966.htm. Accessed July 2008.
cost-effectiveness analysis of peginterferon alfa-2b plus ribavirin for the
35. Binswanger IA, Stern MF, Deyo RA, Heagerty PJ, Cheadle A, Elmore JG,
treatment of naı¨ve patients with chronic hepatitis C. Aliment Pharmacol
et al. Release from prison—a high risk of death for former inmates. N Engl
16. Sullivan SD, Craxi A, Alberti A, Giuliani G, De Carli C, Wintfeld N, et al.
36. Bruno S, Stroffolini T, Colombo M, Bollani S, Benvegnu L, Mazzela G, et
Cost effectiveness of peginterferon alpha-2a plus ribavirin versus interferon
al. Sustained virological response to inteferon-␣ is associated with im-
alpha-2b plus ribavirin as initial therapy for treatment-naive chronic hep-
proved outcome in HCV-related cirrhosis: a retrospective study. HEPATOL-
atitis C. Pharmacoeconomics 2004;22:257-265.
17. Annemans L, Warie H, Nechelput M, Peraux B. A health economic model
37. Veldt BJ, Heathcote EJ, Wedemeyer H, Reichen J, Hofmann WP,
to assess the long term effects and cost-effectiveness of PEG IFN alpha-2a
Zeuzem S, et al. Sustained virologic response and clinical outcomes in
in hepatitis C virus infected patients. Acta Gastroenterol Belg 2004;67:1-8.
patients with chronic hepatitis C and advanced fibrosis. Ann Intern Med
18. Sullivan SD, Jensen DM, Bernstein DE, Hassanein TI, Foster GR, Lee SS,
et al. Cost-effectiveness of combination peginterferon ␣-2a and ribavirin
38. National HCV Prison Coalition. State-by-state HCV treatment guide-
compared with interferon ␣-2b and ribavirin in patients with chronic
lines. Available at: http://www.hcvinprison.org. Accessed July 2008.
hepatitis C. Am J Gastroenterol 2004;99:1490-1496.
39. Federal Bureau of Prisons. Guidelines for the prevention and treatment of
19. Shepherd J, Brodin H, Cave C, Waugh N, Price A, Gabbay J. Pegylated
viral hepatitis. Federal Bureau of Prisons—Clinical Practice Guidelines, Oc-
interferon ␣-2a and -2b in combination with ribavirin in the treatment of
tober 2005. Available at: http://www.bop.gov/news/PDFs/hepatitis.pdf.
chronic hepatitis C: a systematic review and economic evaluation. Health
Technol Assess 2004;8:iii-iv, 1-125.
40. Baillargeon J, Soloway RD, Paar D, Giordano TP, Murray O, Grady J, et
20. Hornberger J, Farci P, Prati D, Zeuzem S, Green J, Patel KK. The eco-
al. End-stage liver disease in a state prison population. Ann Epidemiol
nomics of treating chronic hepatitis C patients with peginterferon ␣-2a (40
kDa) plus ribavirin presenting with persistently normal aminotransferase. J
41. Bennett WG, Inoue Y, Beck JR, Wong JB, Pauker SG, Davis GL. Esti-
mates of the cost-effectiveness of a single course of interferon-alpha 2b in
patients with histologically mild chronic hepatitis C. Ann Intern Med
52. Conjeevaram HS, Fried MW, Jeffers IJ, Terrault NA, Wiley-Lucas TE,
Afdhal N, et al. Peginterferon and ribavirin treatment in African American
42. Macalino GE, Vlahov D, Sanford-Colby S, Patel S, Sabin K, Salas C, et al.
and Caucasian American patients with hepatitis C genotype 1. Gastroen-
Prevalence and incidence of HIV, hepatitis B virus, and hepatitis C virus
infections among males in Rhode Island prisons. Am J Public Health
53. Sterling RK, Hoffman CM, Luketic VA, Sanyal AJ, Contos MJ, Mills AS,
et al. Treatment of chronic hepatitis C virus in the Virginia Department of
43. Vlahov D, Nelson KE, Quinn TC, Kendig N. Prevalence and incidence of
Corrections: can compliance overcome racial differences to response? Am J
hepatitis C virus infection among male prison inmates in Maryland. Eur J
54. Kraus MR, Schafer A, Schottker K, Keicher C, Weissbrich B, Hofbauer I,
44. Armstrong GL, Alter MJ, McQuillan GM, Margold HS. The past inci-
Scheurlen M. Therapy of interferon-induced depression in chronic hepa-
dence of hepatitis C virus infection: implications for the future burden of
titis C with citalopram: a randomized, double-blind, placebo-controlled
chronic liver disease in the United States. H
55. Internet Drug News.com. Antidepressants drug database. Available at:
45. Wong JB, Koff RS. Watchful waiting with periodic liver biopsy versus
http://www.coreynahman.com/antidepressantdrugsdatabase.html. Ac-
immediate empirical therapy for histologically mild chronic hepatitis C.
56. U.S. Department of Justice. Mental health problems of prison and jail
46. Wright M, Grieve R, Roberts J, Main J, Thomas HC, on behalf of the UK
inmates. Bureau of Justice Statistics Special Report, September 2006.
Mild Hepatitis C Trial Investigators. Health benefits of antivital therapy
Available at: http://www.ojp.gov/bjs/pub/pdf/mhppji.pdf. Accessed
for mild chronic hepatitis C: randomized controlled trial and economic
evaluation. Health Technol Assess 2006;10:1-113, iii.
57. Thein HH, Butler TO, Krahn M, Rawlinson W, Levy MH, Kaldor JM, et
47. Younossi ZM, Singer ME, McHutchison JG, Shermock KM. Cost effec-
al. The effect of hepatitis C virus infection on health-related quality of life
tiveness of interferon alpha2b combined with ribavirin for the treatment of
in prisoners. J Urban Health 2006;83:275-288.
chronic hepatitis C. HEPATOLOGY 1999;30:1318-1324.
58. U.S. Department of Justice. Hepatitis testing and treatment in state pris-
48. Drug Topics Red Book. Montvale, NJ: Medical Economics; 2007.
ons. Bureau of Justice Statistics Special Report, April 2004. Available at:
49. U.S. Department of Labor Bureau of Labor Statistics. Consumer price
http://www.ojp.usdoj.gov/bjs/pub/pdf/httsp.pdf. Accessed July 2008.
index calculator. Available at: http://www.bls.gov. Accessed July 2008.
59. Gustafson, Alan. Lawsuit spurs top-rank care to fight disease. Statesman
50. Hoover D, Crystal S, Kumar R. Medical expenditures during the last year
Journal [serial online], Nov. 12, 2007. Available at: http://www.statesman-
of medical expenditures during the last year of life: findings from the
journal.com/apps/pbcs.dll/article?AIDϭ/20071112/NEWS/711120329/
1992-1996 Medicare current beneficiary survey. Health Serv Res 2002;37:
60. The body. The complete HIV/AIDS resource. Available at: http://
51. Wong JB, Bennett WG, Koff RS, Pauker SG. Pretreatment evaluation of
www.thebody.com/content/art31262.html#hcv_inmates.
chronic hepatitis C: risks, benefits and costs. JAMA 1998;280:2088-2093.
Longrove Surgery Travel Health Advice Leaflet The following information will help you to stay healthy on your trip. Please make sure you read it following on from your appointment with us. WATER Diseases can be caught from drinking contaminated water, or swimming in it. Unless you know the water supply is safe where you are staying, ONLY USE (in order of preference) 1. Boiled water2. Bo
Principal Investigator/Program Director (Last, first, middle): BIOGRAPHICAL SKETCH Provide the following information for the key personnel in the order listed for Form Page 2. Follow the sample format on preceding page for each person. DO NOT EXCEED FOUR PAGES. Medical Director, Portuguese Mental Health Clinic; Director, Depression and Anxiety Disorders Research Program, Cambridge Heal
 existing programs that successfully manage tuberculosis,
“hepatitis C,” “treatment,” “cost-effectiveness,” “pris-
human immunodeficiency virus, and other transmittable
ons,” “pegylated-interferon and ribavirin,” “combination
diseases. Treatment could feasibly reduce the incidence of
therapy,” “jails,” and “inmates.”
new hepatitis C virus (HCV) infections and prevent fu-
Using data obtained from these articles, we used the
ture complications from liver disease. Substance abuse
software Treeage Pro Health Module (Williamstown,
and risk reduction counseling could be employed simul-
MA) to construct a decision analysis model employing
taneously, resulting in enduring benefits outside of pris-
Markov simulation (Fig. 1). This allowed us to estimate
the incremental cost-effectiveness ratio (ICER) of combi-
Those who oppose treatment note that therapy is often
nation therapy for hepatitis C in the U.S. prison popula-
interrupted by prison release or transfer, and that contin-
tion and thus compare the strategy of treatment to that of
ued care for hepatitis C after release is often unavailable to
no treatment. The perspective adopted was that of the
what is a largely uninsured population. This could pro-
U.S. prison health care system. We used the generally
mote resistance to therapy or inadequate management of
accepted cost-effectiveness threshold of $50,000 per qual-
treatment-related adverse events. Furthermore, high rates
ity-adjusted life years (QALYs) as the maximum value for
of relapse to injection drug use or other high-risk activity
determining the preferred treatment option.
existing programs that successfully manage tuberculosis,
“hepatitis C,” “treatment,” “cost-effectiveness,” “pris-
human immunodeficiency virus, and other transmittable
ons,” “pegylated-interferon and ribavirin,” “combination
diseases. Treatment could feasibly reduce the incidence of
therapy,” “jails,” and “inmates.”
new hepatitis C virus (HCV) infections and prevent fu-
Using data obtained from these articles, we used the
ture complications from liver disease. Substance abuse
software Treeage Pro Health Module (Williamstown,
and risk reduction counseling could be employed simul-
MA) to construct a decision analysis model employing
taneously, resulting in enduring benefits outside of pris-
Markov simulation (Fig. 1). This allowed us to estimate
the incremental cost-effectiveness ratio (ICER) of combi-
Those who oppose treatment note that therapy is often
nation therapy for hepatitis C in the U.S. prison popula-
interrupted by prison release or transfer, and that contin-
tion and thus compare the strategy of treatment to that of
ued care for hepatitis C after release is often unavailable to
no treatment. The perspective adopted was that of the
what is a largely uninsured population. This could pro-
U.S. prison health care system. We used the generally
mote resistance to therapy or inadequate management of
accepted cost-effectiveness threshold of $50,000 per qual-
treatment-related adverse events. Furthermore, high rates
ity-adjusted life years (QALYs) as the maximum value for
of relapse to injection drug use or other high-risk activity
determining the preferred treatment option.