Tadalafil entfaltet seine Wirkung über eine selektive Hemmung der PDE5, wodurch die Konzentration von cGMP im glatten Muskelgewebe stabil bleibt. Diese biochemische Modulation resultiert in einer langanhaltenden Relaxation der Gefäßwände. Der Wirkstoff wird nach oraler Einnahme effizient resorbiert, mit einer Bioverfügbarkeit von rund 80 %. Seine Halbwertszeit von bis zu 36 Stunden ist innerhalb dieser Substanzklasse außergewöhnlich. Abgebaut wird er in der Leber, hauptsächlich durch CYP3A4, mit anschließender biliärer Exkretion. Typische unerwünschte Wirkungen entstehen durch eine verstärkte Vasodilatation, etwa Kopfschmerzen oder Flush. Pharmakologisch wird cialis generika vor allem durch die verlängerte Wirkungsdauer charakterisiert.
9. wasmuth_umbruchvorlage
EU RO PE AN JOUR NAL OF MED I CAL RE SEARCH
Eur J Med Res (2008) 13: 483-486 I. Holzapfel Publishers 2008
FATAL ACUTE LIVER FAILURE DUE TO REACTIVATION OF HEPATITIS B
FOLLOWING TREATMENT WITH FLUDARABINE/CYCLOPHOSPHAMIDE/
RITUXIMAB FOR LOW GRADE NON-HODGKIN’S LYMPHOMA
J.-C. Wasmuth1, H.-P. Fischer2, T. Sauerbruch1, F. L. Dumoulin1,3
1Department of Internal Medicine I, University Hospital of Bonn, Germany
2Department of Pathology, University Hospital of Bonn, Germany
3Department of Medicine, Gemeinschaftskrankenhaus Bonn, Bonn, Germany
Abstract
ing year a disease relapse was treated with 6 cycles of
Background: Reactivation of chronic hepatitis B in
rituximab (375 mg/m2; day 0), fludarabine (30 mg/m2;
HBsAg carriers is a well known complication of
day 1-3), and cyclophosphamide (250 mg/m2; day 1-3).
chemo therapy. The clinical spectrum ranges from
In addition, the patient had been treated with phen-
asymptomatic hepatitis to fatal hepatic failure. Al-
procoumon for thrombosis of the calf and the
though it impairs the prognosis of cancer treatment, it
popliteal veins diagnosed in March; the treatment had
may be overlooked due to other possible causes of liv-
been stopped when liver function worsened in the be-
ginning of June. Finally, the patient had a past history
Case report: The patient presented with acute liver fail-
of hepatitis B virus (HBV) infection.
ure after 6 cycles of rituximab, fludarabine, and cy-
According to the available information we consid-
clophosphamide for low grade non-hodgkin’s lym-
ered the following differential diagnoses:
phoma. Differential diagnoses were chemotherapy-in-
duced liver failure, autoimmune hepatitis, phenpro-
coumon-induced liver failure and infiltration of the
• Chemotherapy-induced liver failure (veno-occlusive
liver by lymphoma. Finally, reactivation of hepatitis B
with a fibrosing cholestatic pattern was identified. Conclusion: This case reminds clinicians that patients
• Infiltration of the liver by lymphoma
receiving high-intensive chemotherapy or immunosup-
pressive therapy should be screened for HBsAg. Hb-
sAg positive patients should obtain prophylactic an-
tiviral therapy with lamivudine or another substance
Laboratory testing showed a pattern of acute liver fail-
ure, and HBs Ag (Table 1); further workup including
Key words: chemotherapy, reactivation, hepatitis B, liv-
ultrasonography and CT scan as well as bone marrow
biopsy showed no signs of persistent or recurrent
lymphoma. A transjugular liver biopsy showed signs of
highly replicative hepatitis B virus infection with a fi-
brosing cholestatic pattern as assessed by immunohis-
A 55 year-old man was transferred to our tertiary care
university hospital with acute liver failure. Four weeks
before he had been admitted to another hospital with
jaundice, nausea and vomiting. A treatment with pred-
Reactivation of a chronic hepatitis B following chemo -
nisolone (1 mg/kg body weight) had been adminis-
tered for suspected autoimmune hepatitis with positive
smooth muscle antibodies. Because of progressive de-
terioration and development of severe hepatic en-
cephalopathy (grade III) the patient was transferred to
Despite treatment with lamivudine the patient´s clini-
cal condition deteriorated to full-blown liver failure
The information on medical history available upon
with multiorgan failure requiring mechanical ventila-
transfer to our hospital was as follows: the patient had
tion and continuous venovenous hemofiltration. The
indolent Non-Hodgkin-Lymphoma diagnosed in 1992.
patient died from refractory septic shock six days after
It was managed by watchful waiting and eventually
admission to our hospital. Liver transplantation was
with 4 courses of cyclophosphamide, vincristine and
declined by the interdisciplinary transplantation team,
prednisone. From December 2003 to April the follow-
since the patient had underlying lymphoma. Table 1. Course of laboratory values.
29.03. 25.05. 04.06. 10.06. 17.06. Adm.* 21.06. 24.06.
Bilirubin (mg/dl) 5.9 3 5.7 23.6 29.4 29.7g-GT (U/l) 666 737 733 336 192 88AP (U/l) 73 189 796 214 123 ALT (U/l) 86 271 456 1079 1374 281 AST (U/l) 174 393 394 888 1060 467 194Quick (%) 23 18 22 26 24 23 16CHE (U/l) 2361 2123 1726 1406 Creatinine (mg/dl) 0.98 0.9 1.1 4.35LDH (U/l) 249 519 561
Microbiology Hepatitis A
HBs-antigen Positive Positive Anti-HBs Negative Negative Anti-HBc Positive Positive Anti-HBc-IgM Negative Negative HBeAg Negative Positive Anti-HBe n.d. Negative HBV-DNA < 200 cop./ml > 109 cop./ml
Immunology ANA 1:100 (<1:100) LKM Negative (<1:100) SMA 1:200 (<1:100) AMA Negative (<1:100) ANCA Negative (<1:10)
Reference values: Bilirubin 0.1-1.2, g-GT <55, AP 34-131, ALT <45, AST <35, Quick 70-130, CHE 7,000-19,000, Creatinine
Cut off values are given in brackets for immunology parameters. n.d. = not done
ANA = antinuclear antibody, LKM = liver kidney microsome, SLA = soluble liver antigen, SMA = smooth muscle antibody,
AMA = antimitochondrial antibody, ANCA = antinuclear cytoplasmic antibody
of reactivation in HBsAg positive patients is about 20
to 30 % [1, 2]. Several risk factors for reactivation have
Reactivation of chronic hepatitis B in HBsAg carriers
been identified: detectable HBV-DNA before chemo -
is a well known complication of chemotherapy. The
therapy, use of steroids, lymphoma or breast cancer as
clinical spectrum ranges from asymptomatic hepatitis
underlying disease [3], male sex [1]. However, results
to fatal hepatic failure. However, even in its mildest
have been divergent and there is no generally accepted
form with spontaneous recovery, a patient’s prognosis
model for predicting reactivation. This would be of
from cancer may still be impaired from the interrup-
clinical relevance as it is possible to prevent reactiva-
tion in chemotherapy with treatment delay, or prema-
tion by administration of the antiviral drug lamivudine.
ture termination of anticancer therapy. The incidence
Primary prophylaxis with lamivudine has been shown
Fig. 1. Liver histology obtained by transjugular liver biopsy. The hematoxylin-eosin stain (A) shows destruction of large parts of
the parenchyma, marked cholestasis, intralobular fibrosis, and moderate inflammatory infiltration. Immunohistochemistry re-
veals production of HBc (B) and HBs (C) in nearly all hepatocytes. The pattern is consistent with the diagnosis of fibrosing
cholestatic hepatitis due to highly active hepatitis B.
to reduce the frequency and severity of hepatitis flares,
advantages with regard to viral potency and resistance
and to improve survival in HbsAg positive patients [4].
profile. Therefore these substances might be pre-
The largest prospective analysis has found a reduction
ferred, if longer duration of treatment is anticipated.
in reactivation from 24.4 % to 4.6 %, in incidence of
The patient presented had at least two risk factors
hepatitis from 44.6 % to 17.5 %, in severity of hepati-
for reactivation of his hepatitis B virus infection (i. e.
tis and disruption of chemotherapy, although mortality
lymphoma, male sex). In addition, fludarabine is re-
was not affected significantly in this series [5]. A simi-
garded as highly immunosuppressive [10], which fur-
lar reduction could be demonstrated by the same inves-
ther enhances the risk of HBV reactivation [11]. Liver
tigators in breast cancer patients, a group at particular
function tests were elevated already in March, but the
risk for reactivation [6]. Therefore, the recommenda-
workup resulted in the misdiagnosis of autoimmune
tion for prophylactic lamivudine treatment in HBsAg
hepatitis. Retrospective analysis showed prior knowl-
positive patients has been incorporated into the prac-
edge of HBsAg, that was taken into consideration too
tice guidelines of the American Association for the
late though. Thus, the case should remind clinicians
Study of the Liver (AASLD) [7]. Accordingly, patients
that patients receiving high-intensive chemotherapy or
receiving chemo therapy or immunosuppressive therapy
immunosuppressive therapy should be screened for
should undergo screening for HBsAg. Prophylactic an-
HBsAg, at least if they are at risk. HbsAg positive pa-
tiviral therapy with lamivudine is recommended for
tients should obtain prophylactic antiviral therapy with
HBsAg positive patients at the onset of cancer chemo -
lamivudine or another drug active against HBV.
therapy or of a finite course of im muno sup pres sive
therapy, and maintained for 6 months after completion
Competing interests: The authors declare that they have no
of chemo therapy or immuno suppressive therapy [7].
The optimal duration of lamivudine treatment is
not clear. To our knowledge there is no consensus.
The continuation of lamivudine for a variable period
of one to six months after completion of chemothera-
1. Lok AS, Liang RH, Chiu EK, Wong KL, Chan TK, Todd
D. Reactivation of hepatitis B virus replication in patients
py was shown to be equally effective in reducing viral
receiving cytotoxic therapy. Report of a prospective
reactivation [8, 9]. Nevertheless, the AASLD guide-
study. Gastroenterology. 1991 Jan; 100(1): 182-8.
lines recommend a course beginning with the onset of
2. Yeo W, Johnson PJ. Diagnosis, prevention and manage-
chemotherapy and lasting 6 months beyond the com-
ment of hepatitis B virus reactivation during anticancer
pletion of chemotherapy [7]. After the end of lamivu-
therapy. Hepatology. 2006 Feb; 43(2): 209-20.
dine treatment a flare of hepatitis may develop. In the
3. Yeo W, Zee B, Zhong S, Chan PK, Wong WL, Ho WM,
series reported today up to 6 % developed hepatitis af-
Lam KC, Johnson PJ. Comprehensive analysis of risk fac-
ter withdrawal of lamivudine, which was self-limiting
tors associating with Hepatitis B virus (HBV) reactivation
in all cases described so far [5, 8].
in cancer patients undergoing cytotoxic chemotherapy. Br
At the moment there are no sufficient data on new-
J Cancer. 2004 Apr 5; 90(7): 1306-11.
4. Lau GK, He ML, Fong DY, Bartholomeusz A, Au WY,
er anti-HBV agents that might be beneficial in the set-
Lie AK, Locarnini S, Liang R. Preemptive use of lamivu-
ting of chemotherapy or immunosuppression in he-
dine reduces hepatitis B exacerbation after allogeneic
patitis B carriers. It is reasonable to assume that sub-
hematopoietic cell transplantation. Hepatology. 2002 Sep;
stances like adefovir, tenofovir or entecavir might have
5. Yeo W, Chan PK, Ho WM, Zee B, Lam KC, Lei KI,
10. Cheson BD. Infectious and immunosuppressive compli-
Chan AT, Mok TS, Lee JJ, Leung TW, Zhong S, Johnson
cations of purine analog therapy. J Clin Oncol. 1995 Sep;
PJ. Lamivudine for the prevention of hepatitis B virus re-
activation in hepatitis B s-antigen seropositive cancer pa-
11. Picardi M, Pane F, Quintarelli C, De Renzo A, Del Giu-
tients undergoing cytotoxic chemotherapy. J Clin Oncol.
dice A, De Divitiis B, Persico M, Ciancia R, Salvatore F,
Rotoli B. Hepatitis B virus reactivation after fludarabine-
6. Yeo W, Ho WM, Hui P, Chan PK, Lam KC, Lee JJ, John-
based regimens for indolent non-Hodgkin's lymphomas:
son PJ. Use of lamivudine to prevent hepatitis B virus re-
high prevalence of acquired viral genomic mutations.
activation during chemotherapy in breast cancer patients.
Haematologica. 2003 Nov; 88(11): 1296-303.
Breast Cancer Res Treat. 2004 Dec; 88(3): 209-15.
7. Lok AS, McMahon BJ. Chronic hepatitis B. Hepatology. Received: June 15, 2008 / Accepted: July 30, 2008
8. Persico M, De Marino F, Russo GD, Morante A, Rotoli
B, Torella R, De Renzo A. Efficacy of lamivudine to pre-
vent hepatitis reactivation in hepatitis B virus-infected pa-
tients treated for non-Hodgkin lymphoma. Blood. 2002
9. Shibolet O, Ilan Y, Gillis S, Hubert A, Shouval D, Safadi
R. Lamivudine therapy for prevention of immunosup-
pressive-induced hepatitis B virus reactivation in hepatitis
B surface antigen carriers. Blood. 2002 Jul 15; 100(2):
UNITED STATES PATENT AND TRADEMARK OFFICE James D. Weinberger, Laura Popp-Rosenberg and Giselle C. Woo of Fross Zelnick Lehrman & Zissu PC for McNeil-PPC, Inc. Mark J. Liss, Caroline L. Stevens and Michelle L. Calkins of Leydig Voit & Mayer Before Zervas, Kuhlke and Mermelstein, Administrative Trademark Judges. Opinion by Kuhlke, Administrative Trademark Judge: Applicant, Walgreen C
The Israeli Journal of Aquaculture – Bamidgeh 61(1), 2009, 5-26. Full article available to e-journal subscribers Spawning Induction in the Carp: Past Experience and Future Prospects - A Review Z. Yaron1*, A. Bogomolnaya1, S. Drori1, I. Biton2, J. Aizen3, Z. Kulikovsky2 and B. Levavi-Sivan3 1 Department of Zoology, Tel Aviv University, Tel Aviv 69978, Israel 2 Gan Shmuel Fish
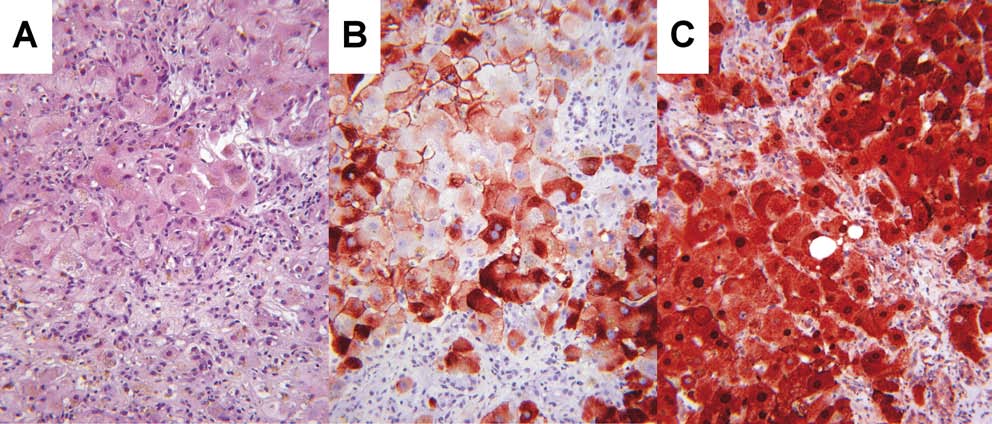 Fig. 1. Liver histology obtained by transjugular liver biopsy. The hematoxylin-eosin stain (A) shows destruction of large parts of
the parenchyma, marked cholestasis, intralobular fibrosis, and moderate inflammatory infiltration. Immunohistochemistry re-
veals production of HBc (B) and HBs (C) in nearly all hepatocytes. The pattern is consistent with the diagnosis of fibrosing
cholestatic hepatitis due to highly active hepatitis B.
Fig. 1. Liver histology obtained by transjugular liver biopsy. The hematoxylin-eosin stain (A) shows destruction of large parts of
the parenchyma, marked cholestasis, intralobular fibrosis, and moderate inflammatory infiltration. Immunohistochemistry re-
veals production of HBc (B) and HBs (C) in nearly all hepatocytes. The pattern is consistent with the diagnosis of fibrosing
cholestatic hepatitis due to highly active hepatitis B.