Tadalafil entfaltet seine Wirkung über eine selektive Hemmung der PDE5, wodurch die Konzentration von cGMP im glatten Muskelgewebe stabil bleibt. Diese biochemische Modulation resultiert in einer langanhaltenden Relaxation der Gefäßwände. Der Wirkstoff wird nach oraler Einnahme effizient resorbiert, mit einer Bioverfügbarkeit von rund 80 %. Seine Halbwertszeit von bis zu 36 Stunden ist innerhalb dieser Substanzklasse außergewöhnlich. Abgebaut wird er in der Leber, hauptsächlich durch CYP3A4, mit anschließender biliärer Exkretion. Typische unerwünschte Wirkungen entstehen durch eine verstärkte Vasodilatation, etwa Kopfschmerzen oder Flush. Pharmakologisch wird cialis generika vor allem durch die verlängerte Wirkungsdauer charakterisiert.
Lodotra.com
Publication summary Efficacy of modified-release versus standard prednisone to reduce duration of morning stiffness of the joints in rheumatoid arthritis (CAPRA-1): a double-blind, randomised controlled trial. Buttgereit F, Doering G, Schaeffler A, et al. Lancet 2008; 371(9608):205-14. Background and key findings
It was proposed that by administering glucocorticoids
of RA compared with baseline. However, this regimen
to rheumatoid arthritis (RA) patients during the night,
was considered to be impractical because it required
instead of the usual morning dosing regimen
regular waking of the patient at 2 a.m. This led to the
(e.g. 6 - 8 a.m.), this may improve the risk:benefit ratio
development of a modified-release (MR) formulation
of this class of drugs. The theory behind this was that
of prednisone which could be taken at bedtime
if the glucocorticoid could be administered in the
(around 10 p.m.) and, after a delay of approximately
early morning hours (approximately 2 a.m.) then this
4 hours, would begin to release the active drug.
would not only mimic the natural circadian rhythm of endogenous cortisol but would also allow the drug
The Circadian Administration of Prednisone in
to act at the most appropriate time point to prevent
Rheumatoid Arthritis (CAPRA-1) Phase III study found
the circadian increases of pro-inflammatory cytokine
that at 12 weeks, the MR prednisone (compared with
concentrations and, consequently, the morning
• a significantly greater relative decrease in the
duration of morning stiffness (P = 0.045);
This concept was confirmed by Arvidson et al.1 who
• a significantly greater relative decrease in serum
demonstrated that the administration of conventional
immediate-release (IR) prednisone at 2 a.m.
• no clinically relevant differences in tolerability
significantly improved the acute morning symptoms
The CAPRA-1 study was set up to assess the efficacy and safety of a modified-release (MR) prednisone tablet compared with immediate-release (IR) prednisone in patients with active rheumatoid arthritis (RA).
A total of 288 patients with active RA were randomised to receive study treatment. As is typical in RA, the patient population in this study were predominantly female (≈ 86%), of white ethnic origin (≈ 99%) and with a mean age of approximately 55 years. Around two-fifths of patients had long-standing disease with duration greater than 10 years, and a further fifth had suffered from RA for five to ten years. They also had a mean 28-joint disease activity score (DAS28) of 5.8.
The majority of patients were receiving a stable dose of disease-modifying antirheumatic drugs (DMARDs; ≈ 95%) and non-steroidal anti-inflammatory drugs (NSAIDs; ≈ 81%). All patients had been receiving glucocorticoids for at least three months with a stable dose of 2.5 mg – 10 mg prednisone (or equivalent) for at least one month before randomisation. The mean daily dose of glucocorticoids was approximately 6.6 mg of prednisone per day (or equivalent).
This paper summary has been written and produced by Mundipharma International Limited
Prescribing information is available on page 3
This was a 12-week, multicentre, randomised, double-blind, active-control ed study. Al patients were randomised to either IR prednisone given in the morning (6 – 8 a.m.) or MR prednisone given in the evening (about 10 p.m.).
Patients continued on the same oral dose of
prednisone that they had taken before the study
(in the range of 3 – 10 mg per day). Therefore the
only difference between the study arms was the
time at which the prednisone was released from
the respective formulations (≈ 6 – 8 a.m. for IR
prednisone and ≈ 2 a.m. for MR prednisone). Primary endpoint: Relative change from baseline in
duration of morning stiffness of the joints at the end
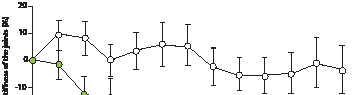
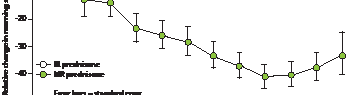
Secondary endpoints: Recurrence of joint stiffness, pain intensity during the day, quality of sleep, DAS28, physician’s global assessment of disease, laboratory variables, health assessment questionnaire, disability index and SF36 scores. Primary endpoint: After 12 weeks of treatment (last observation carried forward method), MR prednisone resulted in a substantially greater decrease in the duration of morning stiffness than IR prednisone [mean relative change -22.7% vs. -0.4%; least square mean difference = 22.4% (95% CI 0.49 – 44.30); P = 0.045]. The absolute difference in the duration of morning stiffness between the treatment groups was 29·2 minutes (95% CI –2·59 to 61·9), in favour of modified-release prednisone (p=0·072). However, the study was not designed to show a significant difference in absolute changes. Secondary endpoints: No clinically or statistically relevant differences were noted between the two treatment groups for secondary variables with the exception of interleukin-6 (IL-6). Serum IL-6 levels decreased with MR prednisone [median relative change -28.6% (range -96.8 to 2018)] but remained constant with IR prednisone [median relative change 0.0% (range -98.1 to 3017)]. The difference between the two groups at week 12 was significant (P = 0.0322).
Figure 2: Relative changes in duration of morning stiffness of the joints from baseline over time
Safety: No clinically relevant differences were observed between the tolerability profiles of MR prednisone and IR prednisone.
Most common adverse events (occurring in 4 or more patients)
MR prednisone is well tolerated, convenient to administer, and produces a clinically relevant reduction in duration of morning stiffness of the joints. This was in addition to all the well known therapeutic effects of IR prednisone.
References:1. Arvidson NG, Gudbjornsson B, Larsson A, et al. The timing of glucocorticoid administration in rheumatoid arthritis.
Lodotra ® 1 mg, 2 mg and 5 mg modified release
and chronic bacterial infections; history of
excretion; increased appetite; weight gain;
prednisone tablets. PRESCRIBING INFORMATION.
tuberculosis. Only use when necessary in patients
reduced glucose tolerance; diabetes mel itus;
with gastrointestinal ulcers; severe osteoporosis and/
hypercholesterolaemia; hypertriglyceridaemia;
Please read the Summary of Product Characteristics or osteomalacia; difficult to control hypertension;
insomnia; headache; cataract; glaucoma; striae
severe diabetes mel itus; current or past psychiatric
rubrae; atrophy; telangiectasia; increased capil ary
Presentation Cylindrical modified release tablets
disorders; glaucoma; corneal ulcers and injuries;
fragility; petechiae; ecchymoses; muscular atrophy
containing prednisone, marked NP and the strength severe ulcerative colitis with imminent perforation;
and weakness; osteoporosis. Other side-effects
on one side. Colours: 1 mg – pale yellowish white,
diverticulitis; entero-anastomoses (immediately
that could be serious are: al ergic reactions;
2 mg – yellowish white, 5 mg – light yellow.
postoperative). Sleep disorder occurs more
disturbed sexual hormone secretion (amenorrhoea,
Indication Treatment of moderate to severe, active frequently compared with conventional IR
impotence); thyroid function disturbance;
rheumatoid arthritis in adults, particularly when
formulation given in the morning. Not recommended depression; euphoria; psychosis; pseudotumor
for patients with galactose intolerance, Lapp lactase cerebri; latent epilepsy; increased predisposition to
Dosage and administration The appropriate dose
deficiency or glucose-galactose malabsorption.
seizures in manifest epilepsy cases; aggravation of
depends on the severity of the condition and the
Depending on treatment duration and the dosage,
corneal ulcer symptoms; promotion of viral, fungal
a negative impact on calcium metabolism must be
and bacterial eye inflammations; hypertension;
Adults: Initial y 10 mg once daily, with subsequent
expected. Osteoporosis prophylaxis is recommended increased risk of arteriosclerosis, thrombosis,
adjustment according to the patient’s response. Take and is particularly important if other risk factors are
vasculitis (also as withdrawal syndrome after long-
at bedtime (around 10 p.m.), with or after evening
present (including familial predisposition, advanced
term therapy); gastrointestinal ulcerations and
meal. Active substance is released 4 – 6 hours after
age, postmenopausal status, insufficient intake of
haemorrhages; pancreatitis; hypertrichosis; steroid
intake, with pharmacological effects starting during
protein and calcium, excessive smoking, excessive
acne; delayed healing of wounds; rosacea-like
the night. Not to be taken in the fasted state. If
alcohol consumption, reduced physical activity).
(perioral) dermatitis; changes in skin pigmentation;
2 – 3 hours have passed after the meal, take with
Interactions Prednisone may interact with: cardiac
hypersensitivity reactions (e.g. drug exanthema) and
a light snack. The tablets should be swal owed
glycosides; saluretics/laxatives; antidiabetics;
aseptic osteonecrosis (humeral and femoral head).
whole and not broken, divided or chewed.
Please refer to the SPC for a ful list of side-effects.
When changing over from the standard regimen
antiphlogistic/antirheumatic agents; salicylates and Package quantities and price Container with
(glucocorticoid administration in the morning) to
indomethacin; non-depolarising muscle relaxants;
30 modified release tablets: 1 mg, 2 mg and 5 mg –
Lodotra administered at bedtime (at about 10 p.m.), atropine and other anticholinergics; praziquantel;
£26.70; Container with 100 modified release tablets:
the same dose (in mg prednisone equivalent) should chloroquine, hydroxychloroquine and mefloquine;
be maintained. Fol owing the change-over, the dose somatropin; oestrogens (e.g. oral contraceptives);
Legal category POM
may be adjusted according to the clinical situation.
liquorice; rifampicin; phenytoin; barbiturates;
Marketing authorisation numbers
Please refer to SPC for information on dose reduction bupropion; primidone; cyclosporine; amphotericine PL 16950/0173 – 0175and discontinuation of therapy.
B; cyclophosphamide; ACE inhibitors; aluminium or
Marketing authorisation holder Napp Childrenandadolescents: Not recommended.
Pharmaceuticals Limited, Cambridge Science Park,
Contra-indications Hypersensitivity to prednisone Pregnancy and lactation Only use at the lowest
Milton Road, Cambridge CB4 0GW, UK. Tel: 01223
or excipients. Please refer to SPC for a full list of
effective dose, if the expected benefits outweigh
424444 Member of the Napp Pharmaceutical Group
For medical information enquiries, please contact
Precautions and warnings Use with caution and Side-effects The most common adverse
appropriate anti-infective therapy in the presence
drug reactions are: moderate leucocytosis;
Date of preparation August 2010
of the fol owing conditions: acute viral infections;
lymphopoenia; eosinopoenia; polycythaemia;
® Lodotra is a registered trade mark of Horizon
HBsAg-positive chronic active hepatitis; 8 weeks
reduced immune defence; masking of infections;
Pharma AG, and is used under licence. NAPP and
before and 2 weeks after live vaccine immunisation; exacerbations of latent infections; adrenal
the ‘NAPP’ device (logo) are registered trade marks
systemic mycoses and parasitoses; poliomyelitis;
suppression; induction of Cushing’s syndrome;
lymphadenitis fol owing BCG inoculation; acute
sodium retention with oedema; increased potassium 2010 Napp Pharmaceuticals Limited. Adverse events should be reported. Reporting forms and information can be found at www.yellowcard.gov.uk. Adverse events should also be reported to Napp Pharmaceuticals Limited on 01223 424444.
For medical information enquires, please contact medicalinformationuk@napp.co.uk
(JTES) Delving: Journal of Technology and Engineering Sciences “Mixed-Solvency” – A novel concept for solubilization of poorly water-soluble drugs Department of Pharmacy, Shri G.S. Institute of Technology and Science Abstract - On the basis of a large number of solubilization experiments on poorly water-soluble drugs, the author is of the opinion that hydrotropy is another type
5-HTP - 5-Hydroxytryptophan aus Griffonia Simplicifolia Hilft beim natürlichen Einschlafen. Verringert die Schmerzempfindlichkeit. Wirkt als natürliches Mittel gegen Depressionen. Lindert Migränekopfschmerzen. Hilft bei der Verminderung von Angst und Stress. Hilft bei der Linderung einiger Symptome von biologischen Störungen im Körper, die durch Alkohol ausgelöst werden, und ist
 This was a 12-week, multicentre, randomised, double-blind, active-control ed study. Al patients were randomised to either IR prednisone given in the morning (6 – 8 a.m.) or MR prednisone given in the evening (about 10 p.m.).
Patients continued on the same oral dose of
prednisone that they had taken before the study
(in the range of 3 – 10 mg per day). Therefore the
only difference between the study arms was the
time at which the prednisone was released from
the respective formulations (≈ 6 – 8 a.m. for IR
prednisone and ≈ 2 a.m. for MR prednisone).
This was a 12-week, multicentre, randomised, double-blind, active-control ed study. Al patients were randomised to either IR prednisone given in the morning (6 – 8 a.m.) or MR prednisone given in the evening (about 10 p.m.).
Patients continued on the same oral dose of
prednisone that they had taken before the study
(in the range of 3 – 10 mg per day). Therefore the
only difference between the study arms was the
time at which the prednisone was released from
the respective formulations (≈ 6 – 8 a.m. for IR
prednisone and ≈ 2 a.m. for MR prednisone).