Tadalafil entfaltet seine Wirkung über eine selektive Hemmung der PDE5, wodurch die Konzentration von cGMP im glatten Muskelgewebe stabil bleibt. Diese biochemische Modulation resultiert in einer langanhaltenden Relaxation der Gefäßwände. Der Wirkstoff wird nach oraler Einnahme effizient resorbiert, mit einer Bioverfügbarkeit von rund 80 %. Seine Halbwertszeit von bis zu 36 Stunden ist innerhalb dieser Substanzklasse außergewöhnlich. Abgebaut wird er in der Leber, hauptsächlich durch CYP3A4, mit anschließender biliärer Exkretion. Typische unerwünschte Wirkungen entstehen durch eine verstärkte Vasodilatation, etwa Kopfschmerzen oder Flush. Pharmakologisch wird cialis generika vor allem durch die verlängerte Wirkungsdauer charakterisiert.
Microsoft powerpoint - unlicensed meds gp talk 0407.ppt
• Introduction• Unlicensed medicines vs ‘off-label’ prescribing• Legislation• Legal responsibility• Professional guidance• Risks and risk management• Take-home points• Questions
• A patient brings a note to your practice from a
paediatric cardiologist in which you are asked to take over the prescribing of an combination product containing hydrochlorothiaizde and spironolactone for a child with a congenital heart malformation.
• Would you agree to take on prescribing responsibility
• What would be consequences for you and the patient
• A consultant in child and adolescent mental health, to
whom you have a referred an 11-year-old child with an autism spectrum disorder who has been displaying violent and aggressive behaviour in school, contacts you to request that you would adopt shared care prescribing for her, now that her condition has been stabilised on treatment with psychosocial therapy and low-dose risperidone.
• Would you agree to take on prescribing responsibility
• What would be consequences for you and the patient
• Medicines Act (1968) – determines licensing
– do not reflect established current knowledge
– do not include well proven uses of a drug
– are at variance e.g. one branded product has two licensed uses but
Legal responsibility lies with person signing the prescription
Manufacturer likely liable only if harm results from a defect in the product
Absence of licensed indication doesn’t imply absence of evidence e.g. spironolactone for heart failure, fluticasone for COPD
May be helpful to recognise a spectrum of risk
– From ‘near-label’ to speculative eccentricity
Consider context – commonplace in children/elderly
What is the extent of the issue within UK
McIntyre J et al. Arch Dis Child 2000;83:498-501
• Single practice study (Midlands, 1997)
– 1175 children (65% <12s on practice list)
poorly represented in clinical trials and the effectiveness of treatment is less certain.
that older patients will receive worthwhile benefits from drug treatment, particularly in terms of reduced risk of stroke.
• Offer patients over 80 years of age the
same treatment as patients over the age of 55, taking account of co-morbidity and polypharmacy
Stewart C. Int J Pharm Pract 2003; 11: R81
• Audit of prescribing of atypicals to 374 patients in
– 48% olanzapine, 28% risperidone, 21% quetiapine, 2.6%
• 53% initiated by specialists, 20% by GP led with advice
• Out of 188 patients who were switched from a typical to an
atypical, 72% complied with NICE guidelines for the switch
Fountoulakis KN. Ann Gen Hosp Pharm 2004; 3: 4
“…the current review proved that data are few and can not really support an evidence based recommendation…. it is impressive that the number of papers without experimental data are four times more in comparison to the experimental ones, and forty times those with controlled double-blind methodology.”
All may not be well in the house of love….
From NPSA website - www.saferhealthcare.org.uk 6th October 2005
Emma died at the age of 5 from complications of adrenal- suppression, she took between 500 and 2000 micrograms of fluticasone every day for several years. She died in 2001. Sheriff’s Investigation: Criticisms of Emma’s treatment and care
– “The GP and the consultant were both aware that Emma was taking high
levels of the inhaled steroid and both believed that even though these high levels of steroid were not ideal, the medication prescribed did not pose a threat to Emma’s health”
Failure to anticipate a rare adverse event
– “.neither Emma’s GP nor her specialist had personal experience of adrenal
suppression or adrenal failure in clinical practice, both believed the risk was sufficiently small to be disregarded”
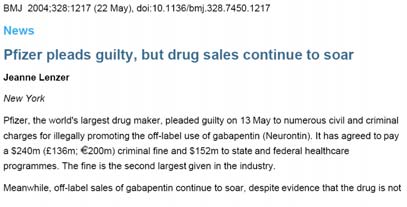
– “GlaxoSmithKline the drug’s manufacturer had promoted the drug as the
drug of choice for managing severe childhood asthma. The advertising slogans stressed the safety of the drug and its use with children”
Off-label prescribing – some common examples
OCD, panic disorder, social phobia, PTSD, GAD
• Products derived from licensed medicines
– e.g. extemporaneously dispensed liquid formulation
• Products unrelated to any licensed medicine
• Products being used in clinical trials
– being imported and used on a named-patient basis
• Little prescribing of unlicensed medicines in mental
• Prescriber carries responsibility for patient’s welfare
• May be called upon to justify actions in event of ADR
• Two main ways through which compensation may be
• Common law duty to take reasonable care
• Act in a way consistent with practice of responsible
body of their peers of similar professional standing (‘The Bolam Principle’)
• Prescribers must understand the product and act
responsibly with reasonable care and skill
• “A doctor is not guilty of negligence if he has acted in
accordance with a practice accepted as proper by a responsible body of medical men skilled in that particular art”
• Product liability arising under the Consumer
• Defective product which does not provide the safety
• Principally affects manufacturers of drugs
Principles of unlicensed prescribing for children (Joint RCPCH/ NPPG)
• Prescribe on the basis of evidence of benefit (and
• Prescribers should have access to good quality
• NHS organisations should support practice
• Be satisfied that an alternative, licensed medicine
• Be satisfied that there is a sufficient evidence base
and/or experience of using the medicine to demonstrate its safety and efficacy
• Take responsibility for prescribing the unlicensed or
off-label medicine and for overseeing the patient’s care, including monitoring and any follow up treatment
• Record the medicine prescribed and the reasons for
choosing this medicine in the patient’s notes. Risk Action
Take comprehensive medication history –
check for previous adequate trial of licensed alternative
Familiarise self with evidence of efficacy
Advise the patient of unlicensed status,
esp where new/investigational medicine or serious risk of ADR
not obtained and
• Unlicensed prescribing is commonplace in mental
• Be aware of licensed indications but…
• Consider licensing issues in context of wider
evidence base, patient preferences, and clinical judgement
• Obtain informed consent whenever possible and
• Monitor closely, withdraw if ineffective
I was a twentysomething barista (and lived) Bert Vandecasteele – 1.2 – 5th of October, 2010 Before moving to Berlin, I didn't even know what a barista was. I probably didn't even know the difference between espresso and regular coffee. But fate had it planned out for me: for about half a year, I'd go into the lion's den. Yes, I would be a twentysomething barista like so many others. I w
Trigeminal Neuralgia RUDOLPH M. KRAFFT, MD, Northeastern Ohio Universities College of Medicine, Rootstown, Ohio Trigeminal neuralgia is an uncommon disorder characterized by recurrent attacks of lancinat- ing pain in the trigeminal nerve distribution. Typically, brief attacks are triggered by talking, chewing, teeth brushing, shaving, a light touch, or even a cool breeze. The pain is nearl


 • Introduction• Unlicensed medicines vs ‘off-label’ prescribing• Legislation• Legal responsibility• Professional guidance• Risks and risk management• Take-home points• Questions
• A patient brings a note to your practice from a
paediatric cardiologist in which you are asked to take over the prescribing of an combination product containing hydrochlorothiaizde and spironolactone for a child with a congenital heart malformation.
• Would you agree to take on prescribing responsibility
• What would be consequences for you and the patient
• Introduction• Unlicensed medicines vs ‘off-label’ prescribing• Legislation• Legal responsibility• Professional guidance• Risks and risk management• Take-home points• Questions
• A patient brings a note to your practice from a
paediatric cardiologist in which you are asked to take over the prescribing of an combination product containing hydrochlorothiaizde and spironolactone for a child with a congenital heart malformation.
• Would you agree to take on prescribing responsibility
• What would be consequences for you and the patient


 • A consultant in child and adolescent mental health, to
whom you have a referred an 11-year-old child with an autism spectrum disorder who has been displaying violent and aggressive behaviour in school, contacts you to request that you would adopt shared care prescribing for her, now that her condition has been stabilised on treatment with psychosocial therapy and low-dose risperidone.
• A consultant in child and adolescent mental health, to
whom you have a referred an 11-year-old child with an autism spectrum disorder who has been displaying violent and aggressive behaviour in school, contacts you to request that you would adopt shared care prescribing for her, now that her condition has been stabilised on treatment with psychosocial therapy and low-dose risperidone.


 What is the extent of the issue within UK
McIntyre J et al. Arch Dis Child 2000;83:498-501
• Single practice study (Midlands, 1997)
– 1175 children (65% <12s on practice list)
poorly represented in clinical trials and the effectiveness of treatment is less certain.
What is the extent of the issue within UK
McIntyre J et al. Arch Dis Child 2000;83:498-501
• Single practice study (Midlands, 1997)
– 1175 children (65% <12s on practice list)
poorly represented in clinical trials and the effectiveness of treatment is less certain.

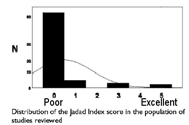


 Fountoulakis KN. Ann Gen Hosp Pharm 2004; 3: 4
“…the current review proved that data are few
Fountoulakis KN. Ann Gen Hosp Pharm 2004; 3: 4
“…the current review proved that data are few 
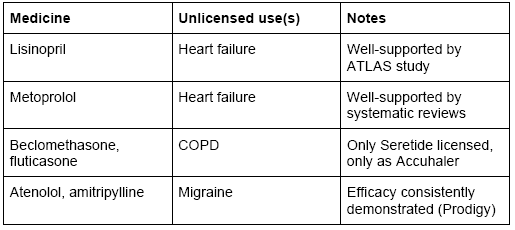

 Off-label prescribing – some common examples
OCD, panic disorder, social phobia, PTSD, GAD
• Products derived from licensed medicines
– e.g. extemporaneously dispensed liquid formulation
• Products unrelated to any licensed medicine
• Products being used in clinical trials
– being imported and used on a named-patient basis
• Little prescribing of unlicensed medicines in mental
Off-label prescribing – some common examples
OCD, panic disorder, social phobia, PTSD, GAD
• Products derived from licensed medicines
– e.g. extemporaneously dispensed liquid formulation
• Products unrelated to any licensed medicine
• Products being used in clinical trials
– being imported and used on a named-patient basis
• Little prescribing of unlicensed medicines in mental


 • Prescriber carries responsibility for patient’s welfare
• May be called upon to justify actions in event of ADR
• Two main ways through which compensation may be
• Common law duty to take reasonable care
• Act in a way consistent with practice of responsible
body of their peers of similar professional standing (‘The Bolam Principle’)
• Prescribers must understand the product and act
responsibly with reasonable care and skill
• “A doctor is not guilty of negligence if he has acted in
accordance with a practice accepted as proper by a responsible body of medical men skilled in that particular art”
• Prescriber carries responsibility for patient’s welfare
• May be called upon to justify actions in event of ADR
• Two main ways through which compensation may be
• Common law duty to take reasonable care
• Act in a way consistent with practice of responsible
body of their peers of similar professional standing (‘The Bolam Principle’)
• Prescribers must understand the product and act
responsibly with reasonable care and skill
• “A doctor is not guilty of negligence if he has acted in
accordance with a practice accepted as proper by a responsible body of medical men skilled in that particular art”


 • Product liability arising under the Consumer
• Defective product which does not provide the safety
• Principally affects manufacturers of drugs
Principles of unlicensed prescribing for children (Joint RCPCH/ NPPG)
• Prescribe on the basis of evidence of benefit (and
• Prescribers should have access to good quality
• NHS organisations should support practice
• Be satisfied that an alternative, licensed medicine
• Be satisfied that there is a sufficient evidence base
and/or experience of using the medicine to demonstrate its safety and efficacy
• Take responsibility for prescribing the unlicensed or
off-label medicine and for overseeing the patient’s care, including monitoring and any follow up treatment
• Record the medicine prescribed and the reasons for
choosing this medicine in the patient’s notes.
• Product liability arising under the Consumer
• Defective product which does not provide the safety
• Principally affects manufacturers of drugs
Principles of unlicensed prescribing for children (Joint RCPCH/ NPPG)
• Prescribe on the basis of evidence of benefit (and
• Prescribers should have access to good quality
• NHS organisations should support practice
• Be satisfied that an alternative, licensed medicine
• Be satisfied that there is a sufficient evidence base
and/or experience of using the medicine to demonstrate its safety and efficacy
• Take responsibility for prescribing the unlicensed or
off-label medicine and for overseeing the patient’s care, including monitoring and any follow up treatment
• Record the medicine prescribed and the reasons for
choosing this medicine in the patient’s notes.


 Risk Action
Risk Action  • Unlicensed prescribing is commonplace in mental
• Be aware of licensed indications but…
• Consider licensing issues in context of wider
evidence base, patient preferences, and clinical judgement
• Obtain informed consent whenever possible and
• Monitor closely, withdraw if ineffective
• Unlicensed prescribing is commonplace in mental
• Be aware of licensed indications but…
• Consider licensing issues in context of wider
evidence base, patient preferences, and clinical judgement
• Obtain informed consent whenever possible and
• Monitor closely, withdraw if ineffective