Tadalafil entfaltet seine Wirkung über eine selektive Hemmung der PDE5, wodurch die Konzentration von cGMP im glatten Muskelgewebe stabil bleibt. Diese biochemische Modulation resultiert in einer langanhaltenden Relaxation der Gefäßwände. Der Wirkstoff wird nach oraler Einnahme effizient resorbiert, mit einer Bioverfügbarkeit von rund 80 %. Seine Halbwertszeit von bis zu 36 Stunden ist innerhalb dieser Substanzklasse außergewöhnlich. Abgebaut wird er in der Leber, hauptsächlich durch CYP3A4, mit anschließender biliärer Exkretion. Typische unerwünschte Wirkungen entstehen durch eine verstärkte Vasodilatation, etwa Kopfschmerzen oder Flush. Pharmakologisch wird cialis generika vor allem durch die verlängerte Wirkungsdauer charakterisiert.
Cost-effectiveness and cost-utility of cognitive therapy, rational emotive behavioral therapy, and fluoxetine (prozac) in treating depression: a randomized clinical trial
Cost-Effectiveness and Cost-Utility of Cognitive Therapy,Rational Emotive Behavioral Therapy, and Fluoxetine(Prozac) in Treating Depression: A RandomizedClinical Trial
Florin A. SavaBabes-Bolyai University, Cluj-Napoca, Romania
Viorel LupuIuliu Hatieganu University of Medicine and Pharmacy,Cluj-Napoca, Romania
Aurora Szentagotai and Daniel DavidBabes-Bolyai University, Cluj-Napoca, Romania
Cost-effectiveness and cost-utility of cognitive therapy (CT), rationalemotive behavioral therapy (REBT), and fluoxetine (Prozac) for majordepressive disorder (MDD) were compared in a randomized clinicaltrial with a Romanian sample of 170 clients. Each intervention wasoffered for 14 weeks, plus three booster sessions. Beck DepressionInventory (BDI) scores were obtained prior to intervention, 7 and 14weeks following the start of intervention, and 6 months followingcompletion of intervention. CT, REBT, and fluoxetine did not differsignificantly in changes in the BDI, depression-free days (DFDs), or
This research was supported by the Albert Ellis Institute, the National Council for Research (Romania),and the Romanian Center for Cognitive and Behavioral Psychotherapies (Grants 113, 33374, and 9,respectively). These organizations had no role in the design and implementation of the study. Details ofprocedures and efficacy findings are provided in David (2006). Correspondence concerning this article should be addressed to: Brian T. Yates, Department ofPsychology, American University, 4400 Massachusetts Avenue, N.W., Washington, DC 20016–8062;e-mail: brian.yates@mac.com
JOURNAL OF CLINICAL PSYCHOLOGY, Vol. 65(1), 36- 52 (2009)
Published online in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/jclp.20550
Costs and Outcomes of Depression Treatments
Quality-Adjusted Life Years (QALYs). Average BDI scores decreasedfrom 31.1 before treatment to 9.7 six months following completion oftreatment. Due to lower costs, both psychotherapies were more cost-effective, and had better cost-utility, than pharmacotherapy: median$26.44/DFD gained/month for CT and $23.77/DFD gained/month forREBT versus $34.93/DFD gained/month for pharmacotherapy, med-ian $/QALYs 5 $1,638, $1,734, and $2,287 for CT, REBT, andfluoxetine (Prozac), respectively. & 2008 Wiley Periodicals, Inc. J ClinPsychol 65:36–52, 2009.
Keywords: depression; cost-effectiveness; cost-utility; pharmacother-apy; CBT; REBT; fluoxetine; DFD; QALY; psychotherapy
Antidepressant medication is promoted as the ‘‘gold standard’’ for treatment ofmajor depressive disorder (MDD; American Psychiatric Association, 2000; Olfson &Klerman, 1993) despite experiments and reviews suggesting that evidence-basedpsychotherapies are at least as effective as pharmacotherapy in treating MDD (e.g.,Antonuccio, Danton, & DeNelsky, 1995; Revicki, Siddique, Frank, Chung, Green,Krupnick et al., 2005; Schulberg, Raue, & Rollman, 2002; Scott, Palmer, Paykel,Teasdale, & Hayhurst, 2003). This may be due to an assumption that medicationcosts less than psychotherapy, which need not be the case. Costs of psychotherapiesare measured correctly according to the duration of therapy and follow-up visits, butcosts of pharmacotherapy are underestimated if limited to doses and monitoringservices delivered over the same period for which psychotherapy was provided (e.g.,12 weeks), given that pharmacotherapy may continue for many months more,possibly through the lifetime of the individual. In addition, if only total monetarycosts are reported, differences found in costs may be due to variation betweencountries in the availability—and thus costs—of therapists relative to therapeuticdrugs.
Psychotherapy researchers studying cognitive-behavioral therapies (CBTs) seem
reluctant to measure, analyze, and report costs, benefits, and cost-effectiveness(Hunsley, 2003; Prigatano & Pliskin, 2003; Yates, 1994). This would be inconsistentwith high-profile endorsements to consider costs, cost-effectiveness, and cost-benefitamong the evidence supporting use of a particular therapy. The AmericanPsychological Association (APA)’s Presidential Taskforce on Evidence-BasedPractice (2006), for example, reported that ‘‘APA endorses multiple types ofresearch evidence (e.g., efficacy, effectiveness, cost-effectiveness, cost-benefit,epidemiological, treatment utilization) that contribute to effective psychologicalpractice.’’ (p. 274). It is, in fact, APA policy since 2002 that evidence on clinicalutility:
y at a minimum y includes attention to generality of effects acrossvarying and diverse patients, therapists, settings, and the interaction ofthese factors; the robustness of treatments across various modes ofdelivery; the feasibility with which treatments can be delivered to patientsin real-world settings; and the costs associated with treatments [italicsadded]. (p. 275).
Journal of Clinical Psychology, January 2009
Measurement and reporting of costs and benefits—critical determinants of
reimbursement policy—may have been left to researchers who consider psychother-apy as at best an adjunctive, and not an alternative, treatment for depression. Inconsistent measurement of costs, and of outcomes, also may prevent conclusivestatements about whether psychotherapy or pharmacotherapy is more effective, lesscostly, or both, relative to each other and relative to usual care.
Additionally, although most studies use a common measure of outcome, the Beck
Depression Inventory (BDI; Beck, Rush, Shaw, & Emery, 1979), that measure maynot be as relevant to policy makers and funders as Depression-Free Days (DFDs;Lave, Frank, Schulberg, & Kamlet, 1998) and Quality-Adjusted Life Years (QALYs;Gold, Siegel, Russell, & Weinstein, 1996; Weinstein & Stason, 1977). Worse yet, thequality of research design also has ranged from randomized clinical trials to self-assignment to psychotherapy or pharmacotherapy (Gabbard, Lazar, Hornberger, &Spiegel, 1997).
Those problems in measurement and design may explain why, relative to studies
that compare costs of different pharmacotherapies for depression, reviews thatcompare costs of pharmacotherapies versus psychotherapies seem more likely toreport conflicting findings. For example Schulberg et al. (2002) and Pirraglia, Rosen,Hermann, Olchanski, and Neumann (2004) concluded that CBT and interpersonalpsychotherapy both were more costly and more effective than were a variety ofcontrol and ‘‘usual care’’ interventions, after reviewing nine and 13 studies,respectively. Pirraglia et al. also found that pharmacotherapies for depression hadlower costs per QALY than did psychotherapies for depression, and therefore bettercost-utility (Levin & McEwan, 2001). However, a review by Barrett, Byford, andKnapp (2005) of 16 studies concluded that pharmacotherapies and psychotherapieshave similar cost-effectiveness in treating depression.
Antonuccio, Thomas, and Danton (1997) found that the effectiveness of
psychotherapies and pharmacotherapies was sufficiently similar to focus theexamination of cost-effectiveness exclusively on possible differences in cost. Antonuccio et al. (1997) estimated that over a 2-year period, pharmacotherapy(fluoxetine or Prozac) resulted in 23% higher costs than individual CBT while alsoestimating that group CBT produced only a 2% cost savings relative to individualCBT. Using a simulation modeling technique, Haby, Tonge, Littlefield, Carter, andVos (2004) concluded that CBT provided by psychologists working in public healthsettings was more cost-effective than was pharmacotherapy using serotonin reuptakeinhibitors (SSRIs) for MDD in children and adolescents. Haby et al. also found thatCBT provided by psychologists working in private settings was similar in cost-effectiveness to pharmacotherapy using selective SSRIs. Cost-effectiveness data frommore empirical studies involving CBT were inconclusive. Revicki et al. (2005) foundno difference in cost-effectiveness between CBT and pharmacotherapy withparoxetine (Paxil) in a randomized clinical trial using a U.S. sample of 267 low-income, minority women. Bower et al. (2000), too, found no difference in cost-effectiveness between CBT, nondirective counseling, and usual care provided by ageneral practitioner, with a sample of 464 patients presenting depression or mixedanxiety and depression.
In an effort to resolve these findings regarding the effectiveness, costs, and cost-
effectiveness of pharmacologic and psychotherapeutic interventions for depression,we assessed and analyzed both the costs and effectiveness of a pharmacotherapy andof two cognitive therapies. Clients diagnosed with MDD were assigned randomly toeither (a) SSRI pharmacotherapy (fluoxetine, Prozac) or (b) the most common
Costs and Outcomes of Depression Treatments
therapy for depression, Cognitive Therapy (CT; see Beck, 1976) or (c) anotherincreasingly common therapy, Rational Emotive Behavior Therapy (REBT; Ellis,1987). As with many other clinical trials for depression treatments (e.g., the NationalInstitute of Mental Health Treatment of Depression Collaborative ResearchProgram; Elkin et al., 1989), and following the American Psychiatric Association(2000) guidelines for treatment of MDD, we excluded a placebo treatment condition. Butler, Chapman, Forman, and Beck’s (2006) review of methodologically rigorousmeta-analyses of CBT showed that it has substantial effect sizes well above thosefound for no-treatment and waiting-list conditions. Butler et al. also noted that‘‘CBT was somewhat superior to antidepressants in the treatment of adultdepression’’ (p. 17).
We chose fluoxetine (Prozac) for the pharmacotherapy because it is one of the mostcommonly prescribed antidepressants and is often described as ‘‘cost-effective:’’Whereas Chisholm, Sanderson, Ayuso-Mateos, and Saxena (2004) found that oldertricyclic antidepressants (TCAs) such as imipramine could be more cost-effectivethan SSRIs—especially in lower income regions–Barrett et al. (2005) concluded thatfluoxetine (Prozac) and other SSRIs appear consistently more cost-effective thanmost TCAs for a variety of patients. Fluoxetine (Prozac) also appears to be saferthan TCAs, in that fluoxetine produces fewer side effects (Mulrow et al., 2000, ascited in Serrano-Blanco et al., 2006) than TCAs and has become relativelyinexpensive (Serrano-Blanco et al., 2006).
We chose Beck’s CT, a common form of CBT, because it is a widely used
psychotherapy for depression with a considerable evidence base (e.g., AmericanPsychiatric Association, 2000; DeRubeis, Gelfand, Tang, & Simons, 1999; Dobson,1989; Hollon, Shelton, & Davis, 1993). CT includes behavioral activation anddysfunctional thought modification as well as identification and structuralmodification of generalized core beliefs presumed to be principle causes of depressivereactions and dysfunctional thinking. We chose a second form of CBT, REBT,because it focuses on different cognitive processes (Ellis, 1987), and it also isaccumulating evidence of its effectiveness (Engels, Garnefsky, & Diekstra, 1993). REBT attempts to change cognitive processes by (a) advocating unconditional self-acceptance; (b) focusing explicitly on reducing secondary problems such asdepression about depression; (c) focusing on demandingness, which seems to bethe core belief involved in MDD; and (d) emphasizing the proximal causes ofnegative feelings (i.e., irrational beliefs).
Our study used a randomized clinical-trial design, measured adherence to treatmentprotocols, and examined and reported attrition rates for each treatment. A separatearticle (David, Szentagotai, Lupu, & Cosman, 2008) has detailed the design,protocols, and some effectiveness findings, written according to ConsolidatedStandards of Reporting Trials, or CONSORT, criteria (Moher, Schulz, & Altman,2001). To facilitate comparison of our findings with other research on psychothera-pies and pharmacotherapies for depression and for other mental illnesses, we reportBDIs, DFDs, QALYs, cost per QALY gained ($/QALY), and cost per DFD gainedper month ($/DFD).
Journal of Clinical Psychology, January 2009
The validity of most cost findings for depression treatments may be limited by
confinement of almost all of this research to four of the most developed countries onEarth: Australia, Canada, the United Kingdom, and the United States of America. Adjustments for differences between nations in currency and cost of living, as well asinflation or deflation since the year cost data were collected, are relatively minorissues. Of more concern are variations between countries in the availability and priceof therapist time. Costs of therapist time may be lower in other countries, even aftermonetary adjustments, because providing therapy may not be valued as highly as areother professions.
To our knowledge, only one study on the costs as well as the effectiveness of
alternative treatments for depression has been conducted in a country not asdeveloped as the aforementioned ‘‘big four.’’ In Chile, psychoeducational treatmentby social workers was found to be more cost-effective than was pharmacotherapy fordepression (Araya, Flynn, Rojas, Fritsch, & Simon, 2006). We attempted to test theexternal validity of both this and similar findings reviewed earlier by conducting ourresearch in a country that is 1 of 40 ‘‘upper middle income economies,’’ according tothe World Bank (2005). Included in these countries are Argentina, Mexico, Poland,Russia, and the nation in which this study was conducted: Romania. Inducted intothe European Union in January 2007, Romania has a per capita Gross DomesticProduct of $9,446. The average gross wage per month in Romania is $545.36 (1418RON or h419.38) based on international exchange rates when data were collected,and $846.06 based on purchasing power parity when data were collected(International Monetary Fund, 2006).
We attempted to improve the potential replicability of cost and cost-effectiveness
findings reported here by itemizing costs, so that the type and amount of each‘‘ingredient’’ resource are available in sufficient detail for other researchers toexamine and convert into current and locally meaningful numbers (Yates, 1996). Costs were itemized for providers, clients, facilities, and materials. The monetaryvalue of each specific resource was obtained for the local economy, as were theamounts and types of each resource used by each treatment. To make our costfindings potentially usable by more interest groups involved in funding decisions, weitemized time spent by consumers as well as providers in treatment and treatment-related activities. Readers who wish to exclude these costs from cost analyses canreadily do so, given the breakdowns provided for time and costs for providers,consumers, and a variety of other treatment resources.
Calculations for statistical power indicated that ns of 52 would detect the mediumeffect size expected from Jacobson et al. (1996) and our experience in clinical trials,with power at .80, a 5 .05, as detailed in David (2006; the manual of the trialpublished in Romania). The 170 adult participants (115 female, 55 male) with nocomorbidity met criteria for MDD according to the Diagnostic and StatisticalManual of Mental Disorders, fourth edition (DSM-IV; American PsychiatricAssociation, 1994), scored at least 20 on the BDI, and scored at least 14 or higheron the Hamilton Rating Scale for Depression (Hamilton, 1967). The support forsuch a standard procedure of selection is presented elsewhere (DeRubeis et al., 1999;Hollon et al., 1993). As detailed in David (2006) and David et al. (2008), attritionduring treatment was 14% in the medication condition, 10% in CT, and 9% in
Costs and Outcomes of Depression Treatments
REBT. Somewhat higher attrition in the medication condition seemed due to sideeffects of medication (i.e., nausea, sexual dysfunction). These dropout rates may belower than usual due to the use of a different population in a different healthcaresystem than is usually the case in published studies, but other researchers havereported reasonably comparable attrition rates of 15% for CBT and 16% formedication (DeRubeis et al., 2005).
Analyses of variance found no significant differences in the following demographic
variables between the three treatment conditions. Participants were a mean 35, 39,and 37 years old in the REBT, CT, and medication conditions (range 5 21–57),respectively. Approximately half had university educations (30, 28, and 31 of the 57,56, and 57 participants in the REBT, CT, and medication conditions, respectively);the remainder had high-school educations. Participants were recruited from fourpublic clinics and research institutes, private practices, and by public-serviceannouncements. Participants were not paid but received the therapy to which theyhad been assigned free of charge. This study was funded by a combination of threeprivate and public research organizations, based in both Romania and the UnitedStates, as detailed in the footnotes. Additional demographics and recruitmentinformation beyond the scope of this article are provided by David et al. (2008).
For persons eligible for participation, the number of previous episodes of
depression was 3.6, 4.0, and 3.9 for the REBT, CT, and medication conditions,respectively. Persons with concurrent psychiatric disorders (i.e., bipolar or psychoticsubtypes of depression, panic disorder, current substance abuse, past or presentschizophrenia or schizophreniform disorder, organic brain syndrome, and mentalretardation; also see Jacobson et al., 1996) were excluded from the study, as werethose already receiving psychotherapy, psychotropic medication, or hospitalizationdue to imminent suicide potential or psychosis.
Participants qualifying for the study provided written informed consent prior to
random assignment to one of the three conditions [i.e., CT, REBT, or fluoxetine(Prozac)]. The pharmacotherapy condition served as the reference condition in thisstudy because it is the ‘‘golden standard treatment’’ for depression according to theAmerican Psychiatric Association (2000). Statistical tests found no significantdifferences prior to treatment in the three conditions, in terms of number of previousepisodes of depression, presence or absence of dysthymia, severity of depression,gender, or marital status (for details, see David, 2006).
A large number of patients were evaluated for the study from 2001 to 2004. To assesstheir eligibility, diagnoses were determined by the Structured Clinical Interview forDSM-IV (First, Spitzer, Gibbon, & Williams, 2001). A clinical psychologist thenevaluated potential participants, the first BDI was administered, and participantswere assigned to conditions. At the middle and the end of the intervention (Weeks 7and 14) and at a 6-month follow-up, participants were administered the BDI by aresearch assistant unaware of the condition to which the participant had beenassigned.
Therapists. Psychotherapies were provided by eight experienced therapists (six
psychologists, two psychiatrists), all certified in CT and REBT, averaging 11 years(range 5 7–14) of postdegree clinical experience. These therapists’ degrees includedthe Romanian equivalents of master’s (n 5 4) and doctoral (n 5 2) degrees for thepsychologists, and the doctor of medicine degree for the two psychiatrists. All had
Journal of Clinical Psychology, January 2009
practiced for at least 7 years following formal training. Pharmacotherapy wasprovided by four psychiatrists with an average 16 years (range 5 14–18) ofpostdegree clinical experience. Manuals elaborated guidelines for each of the threeinterventions. Sessions were audiotaped at random. Tapes were checked for protocolviolation as well as the quality of intervention, finding high levels of fidelity in allthree conditions (David, 2006).
CT. CT was based on the techniques and descriptions in the Beck et al. (1979)
and Beck (1976) manuals. Sessions focused on the identification and structuralmodification of automatic thoughts and generalized core beliefs (schemas) that arepresumed to be the major causes of dysfunctional thinking and depressive reactions(Dowd, 2006; Szentagotai et al., 2006).
REBT. REBT was based on manuals developed by Ellis and others (Ellis, 1962/
1994; Walen, DiGiuseppe, & Dryden, 1992). Treatment focused on the irrationalbeliefs hypothesized to mediate depressive symptoms: demandingness and self-downing. Other core irrational beliefs were approached if identified.
CT, REBT, and pharmacotherapy involved a maximum of 20 individual 50-min
therapy sessions or a maximum of 20 individual 20-min pharmacotherapy sessions,over the 14 weeks allowed for treatment. Clients received an average of 17.5 sessionsof CT, 18.0 sessions of REBT, or 18.0 sessions of fluxoetine monitoring.
Fluoxetine (Prozac). Over 14 weeks of treatment, participants assigned to the
fluoxetine (Prozac) condition attended one session per week with a psychiatrist. Tobetter approximate real-world practice, these sessions were kept shorter than theCBT sessions: After an initial 50-min meeting with the psychiatrist, subsequentsessions were 20 min. Although this may be a longer session duration than iscommon practice in the United States, it is not radically different from the 20- to 30-min biweekly session reported in the literature for clinical research on fluoxetine insome populations (e.g., Treatment for Adolescents with Depression Study Team,2004). Treatment foci were (a) pharmacotherapy management (educating patientsabout medication, adjusting dosage and dosage schedules, inquiring and dealingwith side effects) and (b) clinical management (assessment of the client’s functioningin major areas of life, brief supportive counseling, and limited provision of advice). Fluoxetine (Prozac) typically was taken in the morning. The initial dose of 10 mg/daywas increased to 20 mg/d during Week 1 and to 40 mg/d by Weeks 2 to12. Themaximum dosage allowed was 60 to 80 mg/d (M 5 50.1, SD 5 4.5). During Weeks 12to 14, dosage was reduced again to 20 mg/d for 53% of participants whosedepression improved, in keeping with standard practice (American PsychiatricAssociation, 2000). The remaining participants continued their prescribed doseduring treatment. A maintenance treatment of fluoxetine (Prozac) at 20 to 40 mg/dwas provided during the 6-month follow-up.
Booster sessions. After treatment completion, all participants in the cognitive
conditions were allowed three booster sessions during the subsequent 6 months. Booster sessions could be scheduled at any time, so long as they were at least 1month apart. For participants assigned to the fluoxetine condition, booster sessionsfocused on pharmacotherapy (e.g., inquiring about side effects) and clinical (e.g.,brief supportive counseling and limited advice giving) management. All participantswere asked to not pursue other treatment for depression through the 6-monthfollow-up.
Costs and Outcomes of Depression Treatments
Costs of CT, REBT, and Fluoxetine (Prozac)
Total cost for each treatment condition, and cost per patient in each condition, wascalculated by:
1. measuring the amount of each resource used for a service (e.g., 20 hr of therapy
2. finding the unit cost of each resource (e.g., $100 for each hour of therapy),3. multiplying the amount of each resource used by the cost per unit of that resource
(e.g., 20 hr  $100/hr 5 $2,000 per each patient’s therapy), and
4. summing the costs of each resource to arrive at the total cost, as detailed in Yates
([1980, 1996; e.g., Fals-Stewart, Yates, & Klostermann, 2005).
Romanian cost figures were translated into U.S. dollars according to purchasing
power parity (Gosden & Torgerson, 2002; International Monetary Fund, 2006).
Table 1 lists resources in the far-left column, and, moving from left to right in this
Resource  Procedure matrix (cf. Yates, 1999), the unit measure used for eachresource, the unit cost for each resource, the specific amounts of each resource usedin each treatment condition, and total costs for the total amount of each resourceused for each treatment. For example, on average, a participant assigned in the CTcondition attended a total of 20.41 hr of therapy of a maximum of 23 hr (20 regularand 3 booster sessions). The cost of 1 hr of therapy was estimated at $6.59 based onthe hourly wage of therapists in Romania (a weighted mean based on the fact that oneach psychotherapeutic condition, there were three clinical psychologists and onepsychiatrist who could provide the therapy). Total costs of treatment are listed in thebottom rows of the three right-most columns.
Treatment resources included providers’ time devoted to (a) preparation, (b)
treatment, and (c) assessment (assuming that BDIs would be administered as part oftherapy, even if no research was being conducted). The value of provider time wascalculated per hour from monthly gross wages, including taxes paid by employers. Cost of office space was calculated according to office size, the proportion ofavailable hours that space was used for preparation, treatment, and assessment, andrental costs for local real estate (cf. Yates, 1980, 1999).
Materials and investment costs included manuals and the BDI license and answer
sheets. Cost of fluoxetine (Prozac) was obtained from a retail distributor’s price list,being the best offer from three other retail price lists (a common procedure whenpurchasing goods from public money). Indirect costs such as administration andspace used for activities required by the interventions, such as supervision, werecalculated by multiplying the total of the aforementioned costs by 1.50, reflecting aconservative overhead rate of 50%. Client resources devoted to interventionsincluded time spent in sessions and transportation to and from sessions, multipliedby gross average national income plus fringe benefits, plus transportation costs usingpublic transportation (see Yates, 1980, 1999).
The least expensive treatment was CT (averaging $504.84 per client) and REBT
(M 5 $518.55 per client), followed by fluoxetine (Prozac) (averaging $666.94 perclient). These differences reflect the higher costs associated with medical as opposedto psychological treatments and treatment settings. Moreover, medication was notincluded in overhead calculations because clients rather than providers typicallypurchase and retain medications. Statistical analyses could not be performed on
Journal of Clinical Psychology, January 2009
Table 1Calculation of Psychotherapy and Pharmacology Costs Using a Resources  ProceduresMatrix ($U.S.)
Total cost per treatment 5 no. patients  (Healthcare cost
Total cost per average patient 5 (Healthcare cost 1 Client cost)
Total cost per successful patient 5 Total cost per treatment/n
ÃNote. ‘‘Success’’ refers to the number of recovered or improved patients [42 of 57 for REBT, 39 of 56 forCT, and 36 of 57 for fluoxetine (Prozac)].
these data because cost data were collected for the treatment condition as a wholerather than for the individual client. Future research should examine individualvariability in costs within treatment conditions (Yates, 1996).
Effectiveness of CT, REBT, and Fluoxetine (Prozac)
The three treatments seemed similar in their abilities to reduce depression betweenpretest and posttest, and to maintain this reduction 6 months following completionof treatment. Mean BDI scores for each condition are listed in Table 2. Analysis ofvariance considering type of treatment as a between-participants factor and time(pretest, posttest, and 6-month follow-up) as the within-participants variable foundthat BDI decreased significantly following each of the three treatments, F(1.33,184.83) 5 383.94, po.01, using a Greenhouse–Geisser correction to adjust for
Costs and Outcomes of Depression Treatments
Table 2Means and SDs of Beck Depression Inventory (BDI) Scores for Cognitive Therapy (CT),Rational-Emotive Behavior Therapy (REBT), and Fluoxetine (Prozac)
Table 3Means and SDs for Depression-Free Days (DFDs) and Gain in DFDs per Month
$ per DFDs gained per month, posttest–pretest
$ per DFDs gained per month, follow-up–pretest 49 44.40
violation of sphericity (Field, 2000; Sava, 2004). Post hoc Bonferroni proceduresshowed that both posttest and follow-up BDI scores were significantly lower thanwere pretest BDI scores, but found no significant change between posttest and6-month follow-up. Type of treatment did not affect the decrease in depressivesymptoms, as shown by a nonsignificant Treatment  Time interaction and anonsignificant effect for treatment type, Fso1. Similar findings were evidenced onthe Hamilton Rating Scale for Depression, as detailed in David et al. (2008).
Cost-Effectiveness of CT Versus REBT Versus Fluoxetine (Prozac)
As detailed next, $/DFD was calculated for a client by (a) transforming the client’sBDI scores into DFDs, (b) calculating DFDs gained by the client after intervention,and (c) dividing DFDs gained by the cost of treating a client using the assignedtreatment (from Table 1). Mean $/DFD gained per month are presented in the lasttwo rows of Table 3.
Transforming BDIs into DFDs. Using David’s (2006) norms, BDIr7 indicated
absence of depression, and a BDIZ29 indicated severe depression. Thus, if a clientscored 7 or lower, the client was assumed to have a DFD every day for the month(i.e., 30 days) preceding the assessment and was given a DFD weighting of 1. Similarly, if a client had a BDI score of 29 or higher, the client was assumed to havehad no DFDs during 30 days preceding administration and was given a DFDweighting of zero. Clients with BDIs between 8 and 28 were assigned DFDweightings found by linear interpolation. For example, a BDI of 10 was assigned aDFD weighting of (29À10)/(29À7) 5 19/22 5 .86. DFDs were calculated for the
Journal of Clinical Psychology, January 2009
client by multiplying the client’s DFD weighting by the period (30 days, for thepresent study) preceding assessment (e.g., .86 Â 30 5 25.8 DFDs per month).
DFDs gained per month. DFDs gained per month were found by subtracting
pretest DFDs from posttest DFDs, and by subtracting pretest DFDs from follow-upDFDs. For example, if a client experienced 3 DFDs during the month precedingpretest, and 8 DFDs during the month preceding the posttest, the client gained 5DFDs for the month. Means and SDs for DFDs gained are presented in Table 3. The overall distribution of DFDs was reasonably symmetrical, as suggested by ahistogram and skewness of À.21 and kurtosis of À1.45. These were not reasonablysimilar to the distribution characteristics found for BDIs overall, with skewness of.92 and kurtosis of .40. As expected from the findings for BDI, no significantdifferences were found between treatments in DFDs gained.
Cost per DFD gained per month. For each client, total cost per client in a specific
treatment (Table 1) was divided by DFDs gained for a client to calculate that client’s$/DFD (e.g., $504/18.32 DFDs 5 $27.51 per DFD gained per month, pretest vs. posttest). To avoid division by zero and negative numbers, $/DFD for participantswith no DFD gain (five clients) or DFD decreases (one client) were set as the cost oftreatment for that participant. Possible differences in $/DFD gained per monthbetween treatments were examined with Kruskal–Wallis ANOVAs rather than withparametric ANOVAs because log transformations failed to reduce skewness andheterogeneity of variance (Field, 2000; Sava, 2004). Significant differences in cost-effectiveness were found between treatments for both $/DFD gained per monthbetween pre- and posttest, w2(2) 5 15.59, po.01, and between pretest and follow-up,w2(2) 5 18.77, po.01. Post hoc analyses using mean ranks (Hinkle, Wiersma, & Jurs,1994) revealed that both CT and REBT were significantly more cost-effective thanfluoxetine (Prozac), in $/DFD gained per month, and no significant differences werefound between CT and REBT in $/DFD gained per month, according to the sameprocedures.
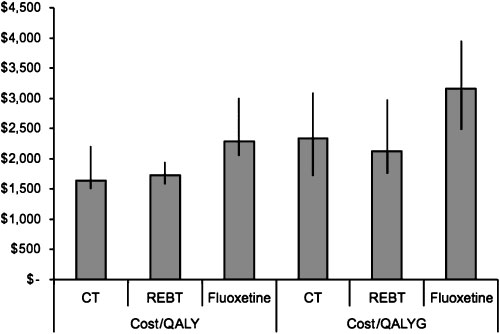
Costs per QALY and QALY gained per year were calculated as detailed by Lave etal. (1998) using utility weights of .40 for severe depression and .90 for recovery fromdepression (Bennett, Torrance, Boyle, & Guscott, 2000; Freed, Rohan, & Yates,2007; Lave et al., 1998; Revicki, Brown, & Palmer, 1995; Revicki & Wood, 1998) (seeFigure 1). Treatments’ $/QALY and $/QALYG were compared by Kruskal–WallisANOVAs for the same reasons presented earlier. Treatments differed significantlyboth in $/QALY, w2(2) 5 35.79, po.01, and in $/QALYG, w2(2) 5 18.66, po.01. Post hoc analyses using mean ranks (Hinkle et al., 1994) found that both CT andREBT had better more cost-utility (i.e., had lower $/QALY and lower $/QALYG)than did fluoxetine (Prozac). No significant differences were found in $/QALY or $/QALYG between CT and REBT. Median $/QALY was $1,638 for CT; $1,734 forREBT; and $2,287 for fluoxetine (Prozac). Median $/QALYG was $2,120 for REBT;$2,342 for CT; and $3,162 for fluoxetine (Prozac).
The present study endeavored to measure and statistically contrast the effectiveness,costs, cost-effectiveness, and cost-utility of CT, REBT, and fluoxetine (Prozac)in treating MDD using a randomized, controlled clinical trial design in a setting
Costs and Outcomes of Depression Treatments
that could yield findings more generalizable to more countries and more peoplethan findings reported to date. In what we have argued to be the moreinternationally representative context of an upper middle income economy, twoforms of CBT, and pharmacotherapy, proved to be effective—equally effective—inreducing depression according to measures advocated by both researchers (BDIs)and policy makers (DFDs and QALYs). CBT even showed some advantage,on some measures, over medication—as found in a variety of other studies (Butleret al., 2006). Both CT and REBT were substantially less expensive than wasfluoxetine (Prozac) pharmacotherapy, a common drug prescribed throughout theworld for depression. We replicated the effectiveness of evidence-based psychothera-pies in treating depression (e.g., Antonuccio et al., 1995; Revicki et al., 2005;Schulberg et al., 2002) and demonstrated that important differences can befound between alternative treatments in their cost-effectiveness and cost-utility. According to median $/QALY, the same effect obtained by paying $100for fluoxetine can be obtained by spending approximately $70 for CBTpsychotherapy [71% less for CT vs. fluoxetine (Prozac), 75% less for REBT vs. fluoxetine (Prozac)].
Cost findings may, of course, be more sensitive than effectiveness findings to
differences in economic context and to cost assessment methods. For instance, lowersalaries for therapists providing psychological interventions in some countries couldtilt cost even more in favor of CBT while higher salaries for therapists or lower costsfor medication could tilt cost-effectiveness and cost-utility findings towardmedication. Certainly, if trained therapists were unavailable but physicians skilledin monitoring dosage and possible side effects of antidepressant medication were,cost could well favor medication over CBT. In addition, shorter or less frequentsessions with psychiatrists would reduce costs of fluoxetine treatment, possiblymarkedly, as could replacement of psychiatrists by nurses or other drug-monitoringprofessionals. The latter was not allowed in the country in which this study wasconducted.
Journal of Clinical Psychology, January 2009
Additionally, new drugs could become less expensive to administer than fluoxetine
(Prozac), making pharmacotherapy as or more inexpensive than CBT, althoughmedical interventions for side effects of any such drugs would be important toinclude in cost calculations. For example, although Vos, Corry, Haby, Carter, andAndrews (2005) found lower cost per disability-adjusted life years (oAUS$ 10,000)using
(AUS$17,000–20,000), they did find similar costs for CBT and TCA medication(which, as noted earlier, has more side effects than SSRIs; Antonuccio et al., 1997). Thus, the question may not be whether one form of therapy is more cost-effective, orhas more cost-utility, than another, but to determine the economic and othercircumstances in which one therapy is more cost-effective than others.
Cost findings also can be affected by the costing perspective adopted
(e.g., provider vs. societal vs. consumer), the type of therapist used (e.g., doctoralvs. master’s vs. paraprofessional), the public or private setting in which therapyis provided, the duration of intervention and maintenance periods, and the overheadrate applied. Of particular interest is that our finding was obtained using aconservative rate of 50% for overhead costs. The lower the rate, the morecompetitive CBT psychotherapy becomes because the cost of medication wasnot included in the overhead. Therefore, reporting details of cost-measurementprocedures and itemizing lists of the types and amounts of resources used ratherthan just reporting a single ‘‘bottom line’’ should facilitate comparisons betweenstudies as well as better understanding of why different researchers arrive at differentcost findings. Measuring costs for each client individually, as done by Fals-Stewart etal. (2005), might show more clearly the relationship between the resources invested intreatment and the outcomes produced for each client as well as better capturing thevariability of costs over clients within the same treatment.
The present study introduces the use of DFDs and QALYs to the depression
research literature, but these findings should be regarded as preliminary andillustrative. Our calculations of DFDs and QALYs assumed that BDI scoresprovided stable estimates of participants’ affect during the rather long periodsbetween BDI administrations. Given that MDD can remit, recur, and otherwisechange suddenly, it can be argued that BDIs provide only a point estimate of whatcan be a highly variable affective state. High variability of affect challenges ourassumption that all points in time between BDI administration, including eachDFD and each quality-adjusted time period, are sufficiently similar to infer, forexample, that all days and time periods between end-of-intervention and follow-upBDIs are similarly free of depression. We hope that future research will assessdepression in a manner that allows more definitive conclusions to be drawnregarding outcome measures that have gained great credence in other researchliteratures (cf. Gold et al., 1996).
The present study is in keeping with long-voiced standards for developing
evidence-based treatments. As advocated by Chambless and Hollon (1988), ‘‘y inevaluating the benefits of a given treatment, the greatest weight should be given toefficacy trials but that these trials should be followed by research on effectiveness inclinical settings and with various populations and by cost-effectiveness research.’’(p. 7). Here, we have reported findings for three classes of variables that providecrucial evidence regarding CBTs as well as a standard pharmacotherapy fordepression: costs, effectiveness (both in terms of depression and QALYs), andcost-effectiveness (both cost of reducing depression and cost of adding QALYs).
Costs and Outcomes of Depression Treatments
In future research, we hope to collect more cost data directly from participants
while they are receiving treatment instead of estimating costs. Follow-ups of 1 to 2years rather than a half-year following completion of treatment could allow furtherdifferences in costs, and in effectiveness, to emerge. Although ethical issues in nottreating persons with MDD argue against it, measurement only and attentionplacebo control conditions could allow more precise calculation of gains in DFD andQALY: To the extent that individuals with MDD spontaneously remit, using pretestscores may exaggerate gain in DFD and QALY that can be attributed to a specifictreatment; however, note that this limitation would not affect costs or absolutevalues for total DFD or QALY. To persuade policy makers to adopt evidence-basedpsychotherapies such as CBT as primary treatments for MDD may require morethan a few studies demonstrating the cost-effectiveness and cost-utility of thosetherapies (Haby et al., 2004). Including measurement of costs and analyses of cost-effectiveness and cost-utility are initial, but necessary, steps in providing moreconsumers with treatments that will benefit them the most with the least impact onlimited healthcare resources.
American Psychiatric Association. (1994). Diagnostic and statistical manual of mental
disorders (4th ed.). Washington, DC: Author.
American Psychiatric Association. (2000). APA practice guidelines for major depressive
disorder (2nd ed.). Washington, DC: Author.
American Psychological Association Presidential Task Force on Evidence-Based Practice.
(2006). Evidence-based practice in psychology. American Psychologist, 61, 271–285.
Antonuccio, D.O., Danton, W.G., & DeNelsky, G.Y. (1995). Psychotherapy versus
medication for depression: Challenging the conventional wisdom with data. ProfessionalPsychology: Research and Practice, 6, 574–585.
Antonuccio, D.O., Thomas, M., & Danton, W.G. (1997). A cost-effectiveness analysis of
cognitive behavior therapy and fluoxetine (Prozac) in the treatment of depression. BehaviorTherapy, 28, 187–210.
Araya, R., Flynn, T., Rojas, G., Fritsch, R., & Simon, G. (2006). Cost-effectiveness of a
primary care treatment program for depression in low-income women in Santiago, Chile. American Journal of Psychiatry, 163, 1379–1387.
Barrett, B., Byford, S., & Knapp, M. (2005). Evidence of cost-effective treatments for
depression: A systematic review. Journal of Affective Disorders, 84, 1–13.
Beck, A.T. (1976). Cognitive therapy for emotional disorders. New York: International
Beck, A.T., Rush, A.J., Shaw, B.F., & Emery, G. (1979). Cognitive therapy of depression.
Bennett, K.J., Torrance, G.W., Boyle, M.H., & Guscott, R. (2000). Cost-utility analysis in
depression: The McSad utility measure for depression health states. Psychiatric Services,51, 1171–1176.
Bower, P., Byford, S., Sibbald, B., Ward, E., King, M., Lloyd, M., et al. (2000). Randomized
controlled trial of non-directive counselling, cognitive-behaviour therapy, and usualgeneral practitioner care for patients with depression: II. Cost effectiveness. British MedicalJournal, 321, 1389–1392.
Butler, A.C., Chapman, J.E., Forman, E.M., & Beck, A.T. (2006). The empirical status of
cognitive-behavioral therapy: A review of meta-analyses. Clinical Psychology Review, 26,17–31.
Journal of Clinical Psychology, January 2009
Chambless, D.L., & Hollon, S.D. (1988). Defining empirically supported therapies. Journal of
Consulting and Clinical Psychology, 66, 7–18.
Chisholm, D., Sanderson, K., Ayuso-Mateos, J.L., & Saxena, S. (2004). Reducing the global
burden of depression. British Journal of Psychiatry, 184, 393–403.
David, D. (2006). Rational treatments: Evidence-based psychological treatments for major
depressive disorders. Bucharest, Romania: Tritonic.
David, D., Szentagotai, A., Lupu, V., & Cosman, D. (2008). Rational emotive behavior
therapy, cognitive therapy, and medication in the treatment of major depressive disorder: Arandomized clinical trial, posttreatment outcomes, and six-month follow-up. Journal ofClinical Psychology, 64, 728–746.
DeRubeis, R.J., Gelfand, L.A., Tang, T.Z., & Simons, A. (1999). Medications versus
DeRubeis, R.J., Hollon, S.D., Amsterdam, J.D., Shelton, R.C., Young, P.R., Salomon, R.M.,
et al. (2005). Cognitive therapy vs medications in the treatment of moderate to severedepression. Archives of General Psychiatry, 62, 409–416.
Dobson, K.S. (1989). A meta-analysis of the efficacy of cognitive therapy for depression.
Journal of Consulting and Clinical Psychology, 57, 414–419.
Dowd, T.E. (2006). What changes in cognitive therapy? The role of tacit knowledge structures.
Journal of Cognitive and Behavioral Psychotherapies, 2, 141–148.
Elkin, I., Shea, T., Watkins, J., Imber, S., Sotsky, S., Collins, J., et al. (1989). The
Research Program: General effectiveness of treatments. Archives of General Psychiatry,46, 971–982.
Ellis, A. (1962/1994). Reason and emotion in psychotherapy. Secaucus, NJ: Birch Lane.
Ellis, A. (1987). A sadly neglected cognitive element in depression. Cognitive Therapy and
Engels, G.I., Garnefsky, N., & Diekstra, R.F.W. (1993). Efficacy of Rational-Emotive
Therapy: A quantitative analysis. Journal of Consulting and Clinical Psychology, 61,1083–1091.
Fals-Stewart, W., Yates, B.T., & Klostermann, K. (2005). Assessing the costs, benefits, cost-
benefit, and cost-effectiveness of marital and family treatments: Why we should and howwe can. Journal of Family Psychology, 19, 28–39.
Field, A. (2000). Discovering statistics using SPSS for Windows. London: Sage.
First, M.B., Spitzer, R.L., Gibbon, M., & Williams, J.B.W. (2001). Interviul Clinic Structurat
pentru tulburarile clinicede pe axa I a DSM (versiunea de cercetare) [Structured clinicalinterview for DSM-IV-TR Axis I Disorders (SCID-I) (research version)]. Cluj-Napoca:Editura RTS.
Freed, M.C., Rohan, K.J., & Yates, B.T. (2007). Estimating health utilities and quality
adjusted life years in seasonal affective disorder research. Journal of Affective Disorders,100, 83–89.
Gabbard, G.O., Lazar, S.G., Hornberger, J., & Spiegel, D. (1997). The economic impact of
psychotherapy: A review. American Journal of Psychiatry, 154, 147–155.
Gold, M.R., Siegel, J.E., Russell, L.B., & Weinstein, M.C. (Eds.). (1996). Cost-effectiveness in
health and medicine. New York: Oxford University Press.
Gosden, T.B., & Torgerson, D.J. (2002). Converting international cost effectiveness data to
UK prices. British Medical Journal, 325, 275–276.
Haby, M.M., Tonge, B., Littlefield, L., Carter, R., & Vos, T. (2004). Cost-effectiveness of
cognitive behavioural therapy and selective serotonin reuptake inhibitors for major
Costs and Outcomes of Depression Treatments
depression in children and adolescents. Australian and New Zealand Journal of Psychiatry,38, 579–591.
Hamilton, M. (1967). Development of a rating scale for primary depressive illness. Journal of
Social and Clinical Psychology, 6, 278–296.
Hinkle, D.E., Wiersma, W., & Jurs, S.G. (1994). Applied statistics for the behavioral sciences
(3rd ed.). Boston: Houghton Mifflin.
Hollon, S.D., Shelton, R.C., & Davis, D.D. (1993). Cognitive therapy for depression:
Conceptual issues and clinical efficacy. Journal of Consulting and Clinical Psychology, 61,270–275.
Hunsley, J. (2003). Cost-effectiveness and medical cost-offset considerations in psychological
service provision. Canadian Psychology, 44, 61–73.
International Monetary Fund. (2006). World economic outlook, Report for selected countries
and subjects, Romania. Available at: http://www.imf.org/external/pubs/ft/weo/2006/02/data/index.aspx
Jacobson, N.S., Dobson, K. S., Truax, P. A., Addis, M. E., Kowener, A. K., Gollan, J. K., et
al. (1996). A component analysis of cognitive-behavioral treatment for depression. Journalof Consulting and Clinical Psychology, 64, 295–304.
Lave, J. R., Frank, R. G., Schulberg, H. C., & Kamlet, M. S. (1998). Cost-effectiveness of
treatments for major depression in primary care practice. Archives of General Psychiatry,55, 645–651.
Levin, H. M., & McEwan, P. J. (2001). Cost-effectiveness analysis (2nd ed.). Thousand Oaks,
Moher, D., Schulz, K.F., & Altman, D.G. (2001). The CONSORT statement: Revised
recommendations for improving the quality of reports of parallel-group randomised trials. The Lancet, 357, 1191–1194.
Olfson, M., & Klerman, G.L. (1993). Trends in the prescription of anti-depressants by office-
based psychiatrists. American Journal of Psychiatry, 150, 571–577.
Pirraglia, P.A., Rosen, A.B., Hermann, R.C., Olchanski, N.V., & Neumann, P. (2004). Cost-
utility analysis studies of depression management: A systematic review. American Journalof Psychiatry, 161, 2155–2162.
Prigatano, G.P., & Pliskin, N.H. (2003). Postscript: Reflections and future directions. In G.P.
Prigatano & N.H. Pliskin, (Eds.), Clinical neuropsychology and cost outcome research: Abeginning (pp. 433–447). New York: Psychology Press.
Revicki, D.A., Brown, R.E., & Palmer, W. (1995). Modeling cost effectiveness of
antidepressant treatment in primary care. Pharmacoeconomics, 8, 524–540.
Revicki, D.A., Siddique, J., Frank, L., Chung, J.Y., Green, B.L., Krupnick, J., et al. (2005).
Cost-effectiveness of evidence-based pharmacotherapy or cognitive behavior therapycompared with community referral for major depression in predominantly low-incomeminority women. Archives of General Psychiatry, 62, 868–875.
Revicki, D.A., & Wood, M. (1998). Health utilities for patients with depression. Journal of
Sava, F.A. (2004). Analiza datelor in cercetarea psihologica [Data analysis in psychological
research]. Cluj-Napoca: Asociatia de Stiinte Cognitive din Romania.
Schulberg, H.C., Raue, P.J., & Rollman, B.L. (2002). The effectiveness of psychotherapy in
treating depressive disorders in primary care practice: Clinical and cost perspectives. General Hospital Psychiatry, 24, 203–212.
Scott, J., Palmer, S., Paykel, E., Teasdale, J., & Hayhurst, H. (2003). Use of cognitive
therapy for relapse prevention in chronic depression. British Journal of Psychiatry, 182,221–227.
Serrano-Blanco, A., Gabarron, E., Garcia-Bayo, I., Soler-Vila, M., Carames, E., Penarrubia-
Maria, M.T., et al. (2006). Effectiveness and cost-effectiveness of antidepressant treatment
Journal of Clinical Psychology, January 2009
in primary health care: A six-month randomised study comparing fluoxetine toimipramine. Journal of Affective Disorders, 91, 153–163.
Szentagotai, A., Schnur, J., DiGiuseppe, R., Macavei, B., Kallay, E., & David, D. (2005). The
organization and the nature of irrational beliefs: Schemas or appraisal. Journal ofCognitive and Behavioral Psychotherapies, 2, 139–158.
Treatment for Adolescents with Depression Study (TADS) Team. (2004). Fluoxetine,
cognitive-behavior therapy, and their combination for adolescents with depression. Journalof the American Medical Association, 292, 807–820.
Vos, T., Corry, J., Haby, M.M., Carter, R., & Andrews, G. (2005). Cost-effectiveness of
cognitive-behavioural therapy and drug interventions for major depression. Australian andNew Zealand Journal of Psychiatry, 39, 683–692.
Walen, S.R., DiGiuseppe, R., & Dryden, W. (1992). A practitioner’s guide to rational-emotive
therapy (2nd ed.). New York: Oxford University Press.
Weinstein, M.C., & Stason, W.B. (1977). Foundations of cost-effectiveness analysis for health
and medical practices. New England Journal of Medicine, 296, 716–721.
World Bank. (2005). Data & statistics, Country groups. Retrieved February 21, 2007, from
http://web.worldbank.org/WBSITE/EXTERNAL/DATASTATISTICS/0,,con-tentMDK:20421402$pagePK:64133150$piPK:64133175$theSitePK:239419,00.html]Up-per_middle_income
Yates, B.T. (1980). Improving effectiveness and reducing costs in mental health. Springfield,
Yates, B.T. (1994). Toward the incorporation of costs, cost-effectiveness analysis, and cost-
benefit analysis into clinical research. Journal of Consulting and Clinical Psychology, 62,729–736.
Yates, B.T. (1996). Analyzing costs, procedures, processes, and outcomes in human services:
An introduction. Thousand Oaks, CA: Sage.
Yates, B.T. (1999). Measuring and improving cost, cost-effectiveness, and cost-benefit for
substance abuse treatment programs [NIH Publication No. 99–4518]. Bethesda, MD:National Institute on Drug Abuse. Available online at: www.nida.nih.gov/IMPCOST/IMPCOSTIndex.html
Registration number 364118 The Arts Specialist Support Agency Limited (A Company Limited by Guarantee and not having a Share Capital) Directors' Report and Financial Statements for the year ended 31 December 2011 The Arts Specialist Support Agency Limited (A Company Limited by Guarantee and not having a Share Capital) Contents Independent Auditors' report to the membersinc
 Costs and Outcomes of Depression Treatments
that could yield findings more generalizable to more countries and more peoplethan findings reported to date. In what we have argued to be the moreinternationally representative context of an upper middle income economy, twoforms of CBT, and pharmacotherapy, proved to be effective—equally effective—inreducing depression according to measures advocated by both researchers (BDIs)and policy makers (DFDs and QALYs). CBT even showed some advantage,on some measures, over medication—as found in a variety of other studies (Butleret al., 2006). Both CT and REBT were substantially less expensive than wasfluoxetine (Prozac) pharmacotherapy, a common drug prescribed throughout theworld for depression. We replicated the effectiveness of evidence-based psychothera-pies in treating depression (e.g., Antonuccio et al., 1995; Revicki et al., 2005;Schulberg et al., 2002) and demonstrated that important differences can befound between alternative treatments in their cost-effectiveness and cost-utility.
Costs and Outcomes of Depression Treatments
that could yield findings more generalizable to more countries and more peoplethan findings reported to date. In what we have argued to be the moreinternationally representative context of an upper middle income economy, twoforms of CBT, and pharmacotherapy, proved to be effective—equally effective—inreducing depression according to measures advocated by both researchers (BDIs)and policy makers (DFDs and QALYs). CBT even showed some advantage,on some measures, over medication—as found in a variety of other studies (Butleret al., 2006). Both CT and REBT were substantially less expensive than wasfluoxetine (Prozac) pharmacotherapy, a common drug prescribed throughout theworld for depression. We replicated the effectiveness of evidence-based psychothera-pies in treating depression (e.g., Antonuccio et al., 1995; Revicki et al., 2005;Schulberg et al., 2002) and demonstrated that important differences can befound between alternative treatments in their cost-effectiveness and cost-utility.