Tadalafil entfaltet seine Wirkung über eine selektive Hemmung der PDE5, wodurch die Konzentration von cGMP im glatten Muskelgewebe stabil bleibt. Diese biochemische Modulation resultiert in einer langanhaltenden Relaxation der Gefäßwände. Der Wirkstoff wird nach oraler Einnahme effizient resorbiert, mit einer Bioverfügbarkeit von rund 80 %. Seine Halbwertszeit von bis zu 36 Stunden ist innerhalb dieser Substanzklasse außergewöhnlich. Abgebaut wird er in der Leber, hauptsächlich durch CYP3A4, mit anschließender biliärer Exkretion. Typische unerwünschte Wirkungen entstehen durch eine verstärkte Vasodilatation, etwa Kopfschmerzen oder Flush. Pharmakologisch wird cialis generika vor allem durch die verlängerte Wirkungsdauer charakterisiert.
Udruzenje-hirurga.ba
CEREBRAL ISCHEMIA PRIOR TO ANEURYSM SURGERY. PREDICTOR OF POOR PROGNOSIS Harun Brkić, Goran Bićanin, Mirza Moranjkić, Mirsad Hodžić ABSTRACT Objective study. We have analyzed the prognostic value of post hemorrhage cerebral isch- emia in aneurismal SAH: the degree of neurological deterioration as graded by the WFNS and GCS scales, the intensity of ischemia as detected by CT scan and timing of surgery. Material and methods. A series of 33 patients, consecutively admitted to our hospital over the last three years, were reviewed retrospectively. The outcome was measured by deter- mining the one-month mortality rate. Results. The mean WFNS scale values were 2.45 for the entire analyzed specimen and 3.40 for the mortality group, respectively. There were no statistically significant differences not- ed between the 2 groups in terms of other factors. Local ischemia was present in 51.5 %, regional ischemia in 30.3 % and global ischemia in 18.2 % patients. Arterial hypertension was noted in 93.9% of all patients and 92.3 % of those who experienced lethal outcome. The percentages of smokers were 87.9 % and 69.2% for the entire group and for the mortality group, respectively. Diabetes mellitus was present in 21.21% of all patients and 23.1% for patients who experienced a lethal outcome. The majority of patients underwent surgery between 4-10 days following the hemorrhage. Conclusion. We conclude that CT confirmed post hemorrhage cerebral ischemia prior to aneurysm surgery and earlier surgery is a major cause of poor prognosis. KEY WORDS: ischemia, post hemorrhage, prognosis. Harun Brkić INTRODUCTION Goran Bićanin
A decreased level of consciousness following the initial subarachnoid hemorrhage (SAH) or
Mirza Moranjkić
early re-bleeding may be caused by a cerebral hematoma, subdural hematoma or hydrocepha-
Mirsad Hodžić
lus. Only by exclusion should it be assumed that the cause is global brain damage as a result of
high pressure and subsequent ischemia. An important notion is that axonal damage may con-
University Clinical Center Tuzla tinue well after the primary injury and extend into the period of delayed cerebral ischemia1.
Ischemia following subarachnoid hemorrhage is a catastrophic complication and a major cause
of in-hospital mortality. The presence of cerebral ischemia after SAH, however, has received
little attention as a prognostic variable. This may be due to the fact that ischemia is a difficult
occurrence to appreciate and quantify on computed
patients with aneurysmal SAH and PCI who were ad-
tomography (CT) scans2. Delayed cerebral ischemia
mitted to the University Hospital Tuzla in Bosnia and
occurs primarily during the first or second week fol-
Herzegovina, in the period between January 2003 and
lowing aneurismal SAH, in up to one-third of patients,
December 2006, all within 4 days after the hemorrhage.
depending on case mix operative regimen3. This oc-
We analyzed 4 additional characteristics of value in the
currence also constitutes a leading cause of disability
after aneurismal SAH. The disability and decrease in
1. Neurological status and CT scan. The patient’s clini-
the number of productive life years caused by SAH is
cal condition had been determined by the World Fed-
comparable to that of cerebral infarction, because of
eration Neurological Scale (WFNS) criteria and Glas-
the relatively young age at onset and poor outcome in
gow Coma Scale (GCS) prior to surgery and one month
SAH4. It is a common belief that a thus far unidenti-
fied factor which induces vasoconstriction and thereby
2. Intensity of cerebral ischemia as seen on the pre-op-
secondary ischemia is introduced in the subarachnoid
erative CT scan graded as either peri-aneurysmal focal
space following the hemorrhage. This report is, in part,
ischemia, regional blood vessel ischemia or global isch-
the result of advances in intensive care management
emia. In our study CT scan was obtained in an interval
that have reduced the damage from cerebral ischemia
between 2 and 7 days after the bleeding.
before and after surgery. There is an abundance of stud-
3. Risk factors for atherosclerosis including: history of
ies regarding the period of greatest risk for developing
prior stroke, arterial hypertension, aspirin use (within
ischemia after subarachnoid hemorrhage. Several stud-
2 weeks before bleed), cigarette smoking, diabetes and
ies have claimed that the highest risk for ischemia is
within the first 24 hours, whereas others have shown
4. Timing of surgery and correlation of surgery with the
the highest risk to be between days 4 and 9 or after day
degree of disability. The timing of surgery was graded as
10. Rates of post-hemorrhage cerebral ischemia (PCI)
surgery performed within 3 days after the hemorrhage,
range between 24% and 35%, when defined by CT scan
between 4-10 days after the hemorrhage and more than
and may be as high as 81% when magnetic resonance
imaging (MRI) is used for diagnosis5. Identifying isch-
All patients were treated according to a standardized
emic lesions after SAH is an important issue because
protocol. Recording the outcome extended for 1 month
the appearance of these lesions on follow-up imaging
correlates with a poor outcome. The effect of ischemic lesions seen on CT scans during the first days of treat-
ment remains unknown, however6. Factors that predict
Over a period of three years we surgically treated 105
the development of ischemic lesions in these patients
patients with aneurismal aubrachnoid hemorrhage. In
have not been defined and clarified7. Recognizing the
33 patients we detected cerebral ischemia by CT scan.
risk factors may have a positive impact on the treat-
Overall mortality was 13 patients. We analyzed 33 pa-
ment. Some studies have shown that the main reason
tients (Group 1) with aneurismal SAH and PCI cere-
for poor clinical results in aneurysm surgery is the exis-
bral ischemia. Fatal outcome was noted in 13 patients
(Group 2). The mean WFNS scale values were 2.45 and 3.4, for the entire analyzed specimen and for the mor-
The goal of this study was to assess the patterns of cere-
bral infarction caused by SAH and to define what clini-cal variables play a role in determining poor outcome in
There were no significant differences between the two
groups in terms of age and sex. Ischemic changes were more intensive in group 2 (Table 2). Most patients
MATERIAL AND METHODS
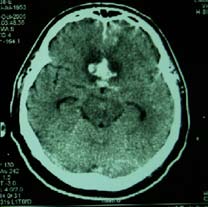
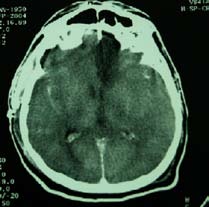
presented with local ischemia. All patients with global
We retrospectively studied a consecutive series of 33
ischemia experienced a poor outcome (Figure 1).
We found no significant influence of smoking, hyper-
Table 1. Results of WFNS and GCS scales
tension, history of stroke or recent use of aspirin and
(33 patients) (13 patients)
Surgery was performed earlier in the mortality group
DISCUSSION
All patients with subarachnoid hemorrhage should
be evaluated and treated on an emergency basis with
maintenance of airway and cardiovascular function. After initial stabilization, patients should be transferred
to centers with neurovascular expertise and preferably
(33 patients) (13 patients)
with a dedicated neurologic critical care unit to opti-
mize care. Once in the critical care setting, the main
goals of treatment are the prevention of re-bleeding, the
prevention and management of vasospasm and delayed ischemia as well as treatment of other medical and neu-rologic complications. All patients in our series were
Table 2. Distribution of patients according to sex,
admitted to the neurosurgical intensive care unit and
vigorously treated prior to and following surgery. It is a
well established fact that secondary brain damage caused
(33 patients) (13 patients)
by delayed cerebral ischemia adversely affects the po-
tential for recovery8-10. The presentation of the ischemic lesions proved to be a strong predictor of the outcome.
Patients who experience cerebral ischemia following
Intensity of
SAH harbor an increased risk for a poor outcome. This
ischemia
may be due to the micro-vascular spasm resulting in
ischemia, induced by blood products in subarachnoid
space, auto-regulatory breakdown or abnormalities
related to ictal cardiovascular arrest. About 50% of pa-tients who survive do not return to their previous level
Figure 1. CT scans depicting local, regional and global ischemic changes.
analyze other complications of surgery, apart from isch-
Table 3. Risk factors for atherosclerosis
emia, that might have had an impact on the outcome.
Data regarding possible risk factors in patients with poor outcome were often lacking. During the CT analy-
(33 patients) (13 patients)
sis, a massive SAH and acute hydrocephalus were noted
in many patients. Studies using MRI have revealed that
delayed ischemic lesions after SAH are usual y bilateral
and multifocal, often involve the frontal lobes and are
CONCLUSION
CT confirmed post hemorrhage cerebral ischemia (PCI), occurring during an initial period upon hemor-
Table 4. Timing of surgery
rhage and before surgery, is a major prognostic factor.
Hypodense lesions detected on CT following subarach-
noid haemorrhage seem to be an independent risk fac-
tor for poor outcome after SAH, and early lesion devel-opment may be more detrimental to clinical outcome
of employment11-13. The prognostic value of the clinical state is stronger than that of previously identified risk
REFERENCES
factors, such as the neurological condition on admis-sion and timing of surgery. This might be explained by
1. Petzold A, Rejdak K, Belli A, Sen J, Keir G, Kitch-
the fact that both the neurological condition and the
en N, et al. Axonal pathology in subarachnoid
timing of surgery change over time and thus depend on
and intracerebral hemorrhage. J Neurotrauma.
the time interval between onset of SAH and admission.
Our data suggest that the severity of the initial ischemia
2. Kreiter KT, Copeland D, Bernardini GL, Bates J,
is an important factor in the final outcome. We did not
Peery S, Claassen J, Connol y ES, Du YE, Stern Y,
find that the presence of risk factors for atherosclerosis
Mayer SA. Predictors of cognitive dysfunction after
and diabetes had a negative impact on outcome. In a re-
subarachnoid hemorrhage. Stroke. 2002; 33: 200–9.
cent study, cigarette smoking was found to increase the
3. Hijdra A, Van Gijn J, Nagelkerke NJ, Vermeulen M,
risk for atherosclerosis and caused difficulties in post
van Crevel H. Prediction of delayed cerebral isch-
operative recovery14. Our study could not support this
emia, rebleeding, and outcome after aneurysmal
finding to a significant degree. Analysis of the utiliza-
subarachnoid hemorrhage. Stroke. 1988;19:1250–6.
tion of aspirin in the aforementioned study may have
4. Weir B, Grace M, Hansen J, Rothberg C. Time course
been unreliable because it was based on data obtained
of vasospasm in man. J Neurosurg. 1978;48: 173–8.
from both patients and their relatives15. Our study did
5. Longstreth WT Jr, Nelson LM, Koepsell TD, van
not support the role of arterial vasospasm in the patho-
Belle G. Clinical course of spontaneous subarach-
genesis of ischemia. No measures of vessel spasm by
noid hemorrhage: a population-based study in King
angiography, TCD or clinical findings were associated
County, Washington. Neurology. 1993;43:712–8.
with the clinical state in the present study. A limiting
6. Siironen J, Porras M, Varis J, Poussa K, Hernesni-
factor in our study is reflected in the fact that we did not
emi J, Juvela S. Early ischemic lesion on computed
tomography: predictor of poor outcome among
13. Vilkki J, Jolst P, Ohman J, Servo A and Heikanen
survivors of aneurysmal subarachnoid hemorrhage.
O. Social outcome related to cognitive performance
Journal of Neurosurgery. 2007;6:1074-9.
and computed tomography findings after surgery
7. Van Gijn J. Subarachnoid haemorrhage. Lancet.
for a ruptured intracranial aneurysm. Neurosur-
8. Janjua N, Mayer SA. Cerebral vasospasm after
14. Lasner TM, Weil RJ, Riina HA, King JT Jr, Zager EL,
subarachnoid hemorrhage. Curr Opin Crit Care.
Raps EC, Flamm ES. Cigarette smoking-induced in-
crease in the risk of symptomatic vasospasm after
9. Rinkel GJE, Feigin VL, Algra A, Feigin VL, Rinkel
aneurysmal subarachnoid hemorrhage. J Neuro-
GJ, Lawes CM et al. Calcium antagonists for aneu-
rysmal subarachnoid haemorrhage. Cochrane Da-
15. Juvela S. Aspirin and delayed cerebral ischemia after
aneurysmal subarachnoid hemorrhage. J Neuro-
10. Van Gijn J, Rinkel GJ. Subarachnoid haemor-
rhage: diagnosis, causes and management. Brain.
16. Kivisaari RP, Salonen O, Servo A, Autti T, Hernesni-
emi J, Ohman J. MR imaging after aneurysmal suba-
11. Ogden JA, Mee E, Henning M. A prospective study
rachnoid hemorrhage and surgery: a long-term fol-
of psychosocial adaptation following subarachnoid
low-up study. Am J Neuroradiol. 2001;22:1143–18.
haemorrhage. Neuropsychol Rehabil. 1994;4:7–30.
17. Sloan MA, Haley EC Jr, Kassell NF, Henry ML, Stew-
12. Powell J, Kitchen N, Heslin J, Greenwood R. Psy-
art SR, Beskin RR, Sevil a EA, Torner JC. Sensitivity
chosocial outcomes at 18 months after good neu-
and specificity of transcranial Doppler ultrasonog-
rological recovery from aneurysmal subarachnoid
raphy in the diagnosis of vasospasm following suba-
haemorrhage. J Neurol Neurosurg Psychiatry.
rachnoid hemorrhage. Neurology. 1989;39:1514–8.
UNIVERSITY OF MELBOURNE DEPARTMENT OF OBSTETRICS & GYNAECOLOGY (ROYAL WOMEN’S HOSPITAL) RESEARCH REPORT 2003 A6 - Authored Books – Other Heffernan M & Quinn MA. 2003. The Gynaecological Cancer Guide Sex Sanity & Survival. Melbourne, Victoria, Australia: Michelle Anderson Publishing Pty Ltd. B1 - Chapters in Research Books Gook D & Edgar DH. 2003. Prac
Evidence based review of escitalopram in treating majordepressive disorder in primary careThomas R. EinarsonThe study aimed to summarize clinical data for43.5%, P = 0.003) but similar to venlafaxine-XR (P = 0.97). escitalopram in the treatment of major depressive disorderResponse rates were superior to placebo (48.7% versusin primary care. Medline, Embase and Cochrane databases43.1%, P <
 We found no significant influence of smoking, hyper-
Table 1. Results of WFNS and GCS scales
We found no significant influence of smoking, hyper-
Table 1. Results of WFNS and GCS scales