Tadalafil entfaltet seine Wirkung über eine selektive Hemmung der PDE5, wodurch die Konzentration von cGMP im glatten Muskelgewebe stabil bleibt. Diese biochemische Modulation resultiert in einer langanhaltenden Relaxation der Gefäßwände. Der Wirkstoff wird nach oraler Einnahme effizient resorbiert, mit einer Bioverfügbarkeit von rund 80 %. Seine Halbwertszeit von bis zu 36 Stunden ist innerhalb dieser Substanzklasse außergewöhnlich. Abgebaut wird er in der Leber, hauptsächlich durch CYP3A4, mit anschließender biliärer Exkretion. Typische unerwünschte Wirkungen entstehen durch eine verstärkte Vasodilatation, etwa Kopfschmerzen oder Flush. Pharmakologisch wird cialis generika vor allem durch die verlängerte Wirkungsdauer charakterisiert.
Microsoft word - 1 - revision weeber icd v3 clean 120118
Parental Permission to Participate in Research Information for parents to consider before allowing their child to take part in this research study IRB Study # Pro00004716
The following information is being presented to help you and your child decide whether or not to be a part of a research study. Please read this information carefully. If you have any questions or if you do not understand the information, we encourage you to ask the researcher.
We are asking you to allow your child to take part in a research study called: The Efficacy of Minocycline in Angelman Syndrome. This study will look at the effects minocycline has in children with Angelman Syndrome (AS). This is a single arm study meaning every participant will receive the study drug and we will compare your child’s performance on behavioral tests before taking the study drug to their performance on the same tests after taking the study drug.
The person who is in charge of this research study is Dr. Edwin Weeber. This person is called the Principal Investigator. However, other research staff may be involved and can act on behalf of the Dr. Weeber. The study neurologist, Maria Gieron, M.D., will perform all medically related study procedures including but not limited to, neurologic examination, laboratory and electroencephalogram test result analysis, and prescription of study medications. During this study your child will undergo behavioral assessments performed by Michael Schoenberg, Ph.D. The study coordinator, Joseph Grieco, M.S., will coordinate the collection of study data, maintain regulatory documents and act as a liaison for you and your child throughout the study process. If you have any questions or concerns, feel free to contact the coordinator anytime by telephone (813) 396-0672 or email, jgrieco1@health.usf.edu.
The research will be conducted on the south Tampa campus of the University of South Florida and at the Tampa General Hospital.
This research is being sponsored in part by the Foundation for Angelman Syndrome Therapeutics. Why is this research being done?
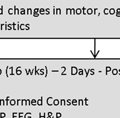
The purpose of this study is to find out the effect of minocycline HCl, a medication normally used as an antibiotic, on the symptoms of Angelman Syndrome. To our knowledge this medication has not yet been used to treat Angelman Syndrome, however, in our laboratory, improvements in cognition, motor function and memory occurred in mice after minocycline was given.
IC Parental Permission Template – Med/SocBeh Rev: 2010-09-03
Why is your child being asked to take part?
We are asking your child to take part in this research study because they have Angelman Syndrome.
In order for your child to be included in the study they must meet the following criteria:
1. Your child’s age must be between the ages of 4 to 12 years old.
2. Your child must have been previously diagnosed with AS by clinical evaluation.
3. Your child’s diagnosis of AS must have a molecular confirmation (e.g. karyotyping, fluorescent in site hybridization, DNA methylation test or sequencing of the ubiquitin protein ligase E3A gene).
4. The participant has a Clinical Global Impressions - Severity score indicating a moderate severity of AS symptoms.
5. You or a guardian, with specific authority to authorize medical treatment, is capable of giving consent on the participant’s behalf.
Should your child take part in this study?
This informed consent form tells you about this research study. You can decide if you want your child to take part in it. This form explains:
• Why this study is being done. • What will happen during this study and what your child will need to do. • Whether there is any chance your child might experience potential benefits from being in the
• The risks of having problems because your child is in this study.
Before you decide:
• Read this form. • Have a friend or family member read it. • Talk about this study with the person in charge of the study or the person explaining the study.
You can have someone with you when you talk about the study.
• Talk it over with someone you trust. • Find out what the study is about. • You may have questions this form does not answer. You do not have to guess at things you
don’t understand. If you have questions, ask the person in charge of the study or study staff as you go along. Ask them to explain things in a way you can understand.
The decision to provide permission to allow your child to participate in the research study is up to you. If you choose to let your child be in the study, then you should sign this form. If you do not want your child to take part in this study, you should not sign the form.
What will happen during this study?
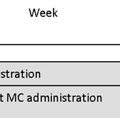
You and your child will be asked to travel to the study site, University of South Florida Health’s South Tampa campus, 3 times (an initial visit and again 8weeks and 16 weeks after enrollment). Each visit will require you and your child to spend 2 days in Tampa in order to complete the required testing.
IC Parental Permission Template – Med/SocBeh Rev: 2010-09-03
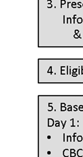
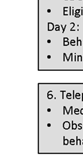
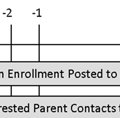
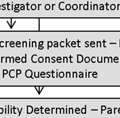
After you have read and then reviewed this informed consent form (ICF), a signed paper copy of the ICF will need to be returned to the study staff. Once the signed ICF has been received, you will be sent a prescreening questionnaire that must be completed by your child’s primary care physician (PCP
completed prescreening form should be returned directly from the PCP to the study coordinator. The prescreening questionnaire will help the study staff determine if it is safe for your child to participate in the study and if your child falls within the inclusion and exclusion criteria prior to traveling to the study site. You will be notified by telephone if your child has been selected to participate in the study.
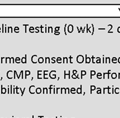
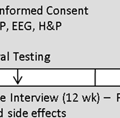
Upon arrival to the study site and before your child receives study medication, your child will undergo baseline testing including a basic metabolic blood screening, an electroencephalogram (EEG), and neurologic examination. The study neurologist will verify the findings stated by your child’s PCP in the prescreening questionnaire and will make the final determination if it is safe for your child to be enrolled in the study. If it is determined safe for your child to continue in the study, several b
be administered by the department of neuropsychology on daay 2. The study coordinator will contact you via telephone throughout the study to give you a chance to ask questions or voice concerns regarding the study. The coordinator will also ask you questions regarding your child’s tolerance to the study drug, behavioral changes you may observe and verify adherence to the dosing regimen.
After 8 weeks of treatment, you and your child will be required to travel to the study site again. During this visit, your child will undergo an EEG, neurologic examination, behavioral testing and be asked to provide a blood sample. The testing will be administered over 2 days and
those performed during the baseline testing.
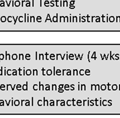
One month after the study medication has been started; the study coordinator will contact you via telephone and conduct a study interview. This interview will assess your child’s tolerance of the study drug and behavioral changes you may observe.
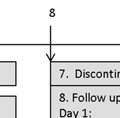
Finally 16 weeks after the first study visit, you and your child will be required to travel to the study site again. During this visit, your child will undergo an EEG, neurologic examination, behavioral testing and be asked to provide a blood sample. The testing will be administered over 2 days and will involve the same tests as those performed during the baseline testing.
IC Parental Permission Template – Med/SocBeh Rev: 2010-09-03
**You should continue to administer any medications your child was receiving at the time of enrollment throughout the study course. However, in the event there is a change in the dosage or the addition of a new medication to their normal medication regimen, the study coordinator should be notified immediately.
During each study visit, your child will be asked to provide a blood sample in order to assess their basic metabolic function (complete metabolic panel & complete blood count) including liver and kidney function. The blood will be obtained by venipuncture, the placement of a needle into a vein to extract blood. During this procedure your child will experience some discomfort in the form of a pricking sensation and/or stinging. This procedure is necessary because the study medication is metabolized and secreted from your child’s body through the liver and kidneys. Ensuring proper function of these organs is essential to avoid toxic levels of study drug in your child’s system.
During each visit, the initial visit and 2 month follow up, your child will undergo the following examinations:
1. A history & physical examination including:
a. Complete medical history – This is done to collect historical information regarding past
treatments, surgery, medical conditions and allergies. The history will most likely be obtained from you, the parent or guardian, but information may be collected from your child as well.
b. Visual Analog Scale - The parent will be asked to evaluate the level of their child’s level
characteristics such as vocalization, motor coordination, ect. They will be asked to place a tick mark on a 10 centimeter line with no ability to the far left and typical ability to the far right. The line will then be measure and the distance from the starting point (left) to the tick mark will be recorded.
c. Focus physical examination – This examination will require a board certified pediatric
neurologist to physically touch your child. During the examination the physician will collect:
i. Vital Signs – body temperature, heart rate, respiratory rate and blood pressure
ii. Organ systems review of the cardiovascular, respiratory and abdominal systems
iii. Clinical Global Impressions – Severity scale. This test does not require any
participation from your child. The score will be based on the history and physical examination completed by the study neurologist.
iv. Neurologic examination – muscle tone, locomotion and gait and tremors or
2. Electroencephalogram (EEG) – In some cases, your child may have already had an EEG;
however, to maintain the integrity of the study, another EEG will be performed. This test will be performed at the Tampa General Hospital by hospital staff members. The test will require electrodes to be attached to your child’s head and will last for approximately 30 minutes. Children with AS have a distinctive EEG signature and we hope the administration of study drug will result in a more normal EEG signature.
3. Developmental Assessments - On the second day of testing, your child will undergo behavioral
testing administered by the Department of Neuropsychology at the University of South Florida Health. Your child’s ability will be assessed according to the following tests.
IC Parental Permission Template – Med/SocBeh Rev: 2010-09-03
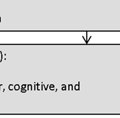
4. Bayley Scales of Infant and Toddler Development, 3rd edition (BSID-III) - These standard
series of measurements is used to assess the fine and gross motor skills, receptive and expressive language skills and cognitive development of infants and toddlers from age 0-3. a. Bayley Scales may be replaced by Differential Ability Scale (DAS-II) in the more
developmentally advanced participant, those who exceed specific scores on the BSID-III as determined by the department of neuropsychology. Like the BSID-III, the DAS-II provides an assessment of the participant’s cognitive abilities. The diagnostic subtests measure a variety of abilities including verbal and visual memory, recall, visual recognition, processing speed, phonological processing and understand of basic number concepts.
5. Vineland Adaptive Behavior Scale, 4th edition (Vineland-II) - This test is to measure the
adaptive behaviors; the ability to adapt to changes in one’s environment, learn new everyday skills and level of independence.
6. Aberrant Behavior Checklist - Community version (ABC – Community) - This behavior
rating scale utilizes direct observation to measure behavior problems in those with mental retardation. The checklist evaluates irritability, lethargy, stereotypic behavior, hyperactivity, inappropriate speech and provides a raw score for each domain.
a. Preschool Language Scale, Fourth Edition (PLS-4) - This test is used to evaluate the
development of expressive and receptive language development. It also can be used to assess behaviors considered to be language precursors.
How many other people will take part?
This study will include only one study site, the University of South Florida. About 24 individuals will take part in this study.
What other choices do you have if you decide not to let your child to take part?
If you decide not to let your child take part in this study, that is okay. Instead of being in this research study your child can choose not to participate.
Alternatives to participating in the study include:
• Participation in other clinical trials.
Will your child be compensated for taking part in this study?
You will receive no payment or other compensation for taking part in this study.
What will it cost you to let your child take part in this study?
It will not cost you anything to let your child take part in the study. The study drug and all tests outlined in this document are being paid by the study sponsor. However, routine medical care for your child’s condition (care he/she would have received whether or not they were in this study) will be charged to
IC Parental Permission Template – Med/SocBeh Rev: 2010-09-03
you or your insurance company. You may wish to contact your insurance company to discuss this further.
What are the potential benefits to your child if you let him / her take part in this study?
We do not know if this study will help children with Angelman Syndrome that is why we are doing this study. By volunteering, you and your child are helping us learn more about what does or does not help individuals with this condition. What we learn may help others in the future.
What are the risks if your child takes part in this study?
While the risks of severe side effects are low, there are some known risks associated with taking the study medication, (Minocyline). It is important to note, Minocyline, has not been approved by the FDA for use in children younger than 8 years old. The medication has the ability to cause permanent discoloration of the teeth in children that have not yet developed “adult” teeth. The study staff has put into place a procedure to assess the color of your child’s teeth at each study visit. We will inform you immediately if a change in color has occurred so that you can decide if your child should continue to participate. Get emergency medical help from a hospital if you observe any signs of an allergic reaction to minocycline including: hives; difficulty breathing; swelling of the face, lips, tongue, or throat.
Call your primary care physician at once if you have a serious side effect such as:
• stomach cramps, diarrhea that is watery or bloody; • flu symptoms, sores in your mouth and throat; • pale or yellowed skin, weakness, dark colored urine, unusual bleeding (nose, mouth, vagina, or
rectum), purple or red pinpoint spots under your skin;
• fever, skin rash, bruising, severe tingling or numbness, muscle weakness, • upper stomach pain, loss of appetite, jaundice (yellowing of the skin or eyes); • chest pain, irregular heart rhythm, cough, wheezing, feeling short of breath; • confusion, vomiting, swelling, weight gain, urinating less than usual or not at all; • headache or pain behind your eyes, ringing in your ears, vision problems; • joint pain or swelling with fever, swollen glands, muscle aches, general ill feeling, unusual
thoughts or behavior, and/or seizure (convulsions); or
• severe skin reaction -- fever, sore throat, swelling in your face or tongue, burning in your eyes,
skin pain, followed by a red or purple skin rash that spreads (especially in the face or upper body) and causes blistering and peeling.
Less serious minocycline side effects may include:
• dizziness, tired feeling, spinning sensation; • joint or muscle pain; • discoloration of skin or nails; • mild nausea, mild diarrhea, upset stomach; • mild skin rash or itching; • swollen tongue, discoloration of your gums; or
IC Parental Permission Template – Med/SocBeh Rev: 2010-09-03
If you suspect your child has any of the problems listed above, contact your primary care physician immediately. If possible, you should show your copy of this informed consent document to them. Once your child has received the necessary medical attention, contact the principal investigator or study coordinator and let them know of the events your child has experienced and the treatment they received. You can reach the study staff at all hours, any day of the week by calling (813) 421-1656.
If at any time you have questions regarding the study or study medication you should call the study staff member on call at (813) 421-1656 and they can direct you to the appropriate resource to answer your question.
TAMPA GENERAL INJURY STATEMENT (CHILD)
In the event your child suffers an injury or illness as a result of participating in this research study, please be aware that immediate, short-term medical treatment for the injuries or illness will be available to you from Tampa General Hospital. You will not be responsible for the costs related to these injuries. No compensation will be offered. You are not giving up any legal rights by signing this form. If you believe your child has experienced a reaction to the study drug/device or has been injured as a result of research procedures performed at Tampa General Hospital, please contact the Department of Risk Management at (813) 844-7666.
Conflict of Interest Statement
No conflict of interest exists for any of the investigators or staff involve in this study.
Authorization to Use and Disclose Protected Health Information Who will see your child’s health information?
In this research study, we use and share your child’s health information to the extent authorized (permitted) by you. We know that this information is private. The federal privacy regulations of the Health Insurance Portability & Accountability Act (HIPAA) protect your identifiable health information. If you authorize us to use your child’s information we will protect it as required by law.
This research is conducted at the University of South Florida (USF). By signing this form, you are permitting USF to use personal health information collected about your child for research purposes within the USF health care system. You are also allowing USF to share your child’s personal health information with individuals or organizations other than USF who are also involved in the research and listed below.
Who will disclose (share), receive, and/or use your child’s information?
To conduct this research, USF and the people and organizations may use or share your child’s information. They may only use and share your child’s information:
IC Parental Permission Template – Med/SocBeh Rev: 2010-09-03
• With the people and organizations on this list; • With you or your personal representative; and • As allowed by law.
In addition to the people and organizations listed below in the Privacy and Confidentiality section of this document, the following groups of people may also be able to see information about your child and may use the information to conduct the research:
• The medical staff that takes care of your child and those who are part of this research study; • Each research site for this study. This includes the research and medical staff at each site and
• Any laboratories, pharmacies, or other individuals and organizations that use your child’s health
information as part of the approved plan for this study;
• Data Safety Monitoring Boards or others who monitor the data and safety of the study.
Who else can use and share this information? Anyone listed above may use consultants in this research and for the purpose of this study, may share your child’s information with them. If you have questions about who they are, you should ask the study team. Individuals who receive your child’s health information for this research study may not be required by the HIPAA Privacy Rule to protect it and may share your child’s information with others without your permission. They can only do so if permitted by the laws governing them. For example, the study sponsor may share your child’s information with others. If the sponsor or others share your child’s information, this information may no longer be protected under the HIPAA Privacy Rule. How will my information be used? By signing this form, you are giving permission to use and/or share your child’s health information as described in this document for any and all study/research related purposes. Your authorization to use your child’s health information will not expire unless you revoke it in writing.
As part of this research, USF may collect, use, and share the following information:
• Your child’s whole research record • All of your child’s past, current or future medical and other health records held by USF, other
health care providers or any other site affiliated with this study. This includes, but is not limited to, their complete medical history, physical examination, EEG results and behavioral assessments.
Your Rights: You can refuse to sign this form. If you do not sign this form your child will not be able to take part in this research study and therefore not be able to receive the research related interventions. However, your child’s health care outside of this study and benefits will not change. How Do I Withdraw Permission to Use My Child’s Information?
You can revoke this form at any time by sending a letter clearly stating that you wish to withdraw your authorization to use of your child’s health information in the research. If you revoke your permission:
• You child will no longer be a participant in this research study;
IC Parental Permission Template – Med/SocBeh Rev: 2010-09-03
• We will stop collecting new information about your child; • We will use the information collected prior to the revocation of your authorization. This
information may already have been used or shared with other, or we may need it to complete and protect the validity of the research; and
• Staff may need to follow-up with your child if there is a medical reason to do so.
While we are conducting the research study, we cannot let you see or copy the research information we have about your child. Privacy and Confidentiality
We will keep your child’s study records private and confidential. Certain people may need to see your child’s study records. By law, anyone who looks at your child’s records must keep them completely confidential. The only people who will be allowed to see these records are:
• The research team, including the Principal Investigator, study coordinator, research nurses, and
all other research staff.
• Certain government and university people who need to know more about the study. For
example, individuals who provide oversight on this study may need to look at your records. This is done to make sure that we are doing the study in the right way. They also need to make sure that we are protecting your rights and your safety.
• Any agency of the federal, state, or local government that regulates this research. This includes
the Food and Drug Administration (FDA), Florida Department of Health, and the Department of Health and Human Services (DHHS) and the Office for Human Research Protection (OHRP).
• The USF Institutional Review Board (IRB) and its related staff, who have oversight
responsibilities for this study, staff in the USF Office of Research and Innovation, USF Division of Research Integrity and Compliance, and other USF offices who oversee this research.
• By signing this form, you are permitting Tampa General Hospital to receive, use, and share
personal health information collected about you for research purposes within Tampa General Hospital health care system. You are also allowing Tampa General Hospital to share your personal health information with other individuals or organizations who are also involved in this research.
We may publish what we learn from this study. If we do, we will not include your child’s name. We will not publish anything that would let people know who your child is. What happens if you decide not to let your child take part in this study?
You should only let your child take part in this study if both of you want to. You or your child should
IC Parental Permission Template – Med/SocBeh Rev: 2010-09-03
not feel that there is any pressure to take part in the study to please the study investigator or the research staff.
If you decide not to let your child take part:
• Your child will not be in trouble or lose any rights he/she would normally have. • You child will still get the same services he/she would normally have.
You can decide after signing this informed consent form that you no longer want your child to take part in this study. We will keep you informed of any new developments which might affect your willingness to allow your child to continue to participate in the study. However, you can decide you want your child to stop taking part in the study for any reason at any time. If you decide you want your child to stop taking part in the study, tell the study staff as soon as you can.
• We will tell you how to stop safely. We will tell you if there are any dangers if your child stops
• If you decide to stop, your child can continue receiving his/her regular medical attention from
Even if you want your child to stay in the study, there may be reasons we will need to withdraw him/her from the study. Your child may be taken out of this study if we find out it is not safe for your child to stay in the study or if your child is not coming for the study visits when scheduled. We will let you know the reason for withdrawing your child’s participation in this study.
You can get the answers to your questions, concerns, or complaints.
If you have any questions, concerns or complaints about this study, Dr. Edwin Weeber at (813) 396-9995
If you have questions about your child’s rights, general questions, complaints, or issues as a person taking part in this study, call the USF IRB at (813) 974-5638.
Consent for My Child to Participate in this Research Study
And Authorization to Collect and Use His/Her Health Information for Research.
It is up to you to decide whether you want your child to take part in this study. If you want your child to take part, please read the statements below and sign the form if the statements are true. I freely give my consent to let my child take part in this study and authorize that my child’s health information as agreed above, be collected/disclosed in this study. I understand that by signing this form I am agreeing to let my child take part in research. I have received a copy of this form to take with me.
**The signature of both parents is required for participation in this study.**
IC Parental Permission Template – Med/SocBeh Rev: 2010-09-03
Statement of Person Obtaining Informed Consent
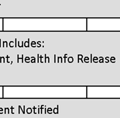
I have carefully explained to the parent of the child taking part in the study what he or she can expect from their child’s participation. I hereby certify that when this person signs this form, to the best of my knowledge, he/ she understands:
• What the study is about; • What procedures/interventions/investigational drugs or devices will be used;
• What the potential benefits might be; and
I can confirm that this research subject speaks the language that was used to explain this research and is receiving an informed consent form in the appropriate language. Additionally, this subject reads well enough to understand this document or, if not, this person is able to hear and understand when the form is read to him or her. The parent signing this form does not have a medical/psychological problem that would compromise comprehension and therefore makes it hard to understand what is being explained and can, therefore, give legally effective informed consent. The parent signing this form is not under any type of anesthesia or analgesic that may cloud their judgment or make it hard to understand what is being explained and, therefore, can be considered competent to give permission to allow their child to participate in this research study.
IC Parental Permission Template – Med/SocBeh Rev: 2010-09-03
Chapitre 1 LA MALADIE DE PARKINSON ET SES TRAITEMENTS Ont contribué à l’élaboration, la rédaction et la révision de cette section : Line Beaudet Chantal Beauvais Sylvain Chouinard Manon Desjardins Michel Panisset Emmanuelle Pourcher Valérie Soland Maladie de Parkinson Thalamus Substance noire Tronc cérébral Noyau sous-thalamique Globus pallidus Putamen Noyau ca
Weekly Market Review What an interesting week. I feel like I need Dramamine to deal with all the quick ups and downs in the market. We don't believe that yesterday was anything more than an oversold rally that will not last. Today's activity kind of confirms that. We used the up day yesterday to get even more conservative and we are in a great position today across the board – we
 Parental Permission to Participate in Research
Parental Permission to Participate in Research 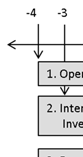
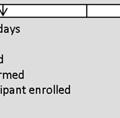

 After you have read and then reviewed this informed consent form (ICF), a signed paper copy of the ICF will need to be returned to the study staff. Once the signed ICF has been received, you will be sent a prescreening questionnaire that must be completed by your child’s primary care physician (PCP
completed prescreening form should be returned directly from the PCP to the study coordinator. The prescreening questionnaire will help the study staff determine if it is safe for your child to participate in the study and if your child falls within the inclusion and exclusion criteria prior to traveling to the study site. You will be notified by telephone if your child has been selected to participate in the study.
Upon arrival to the study site and before your child receives study medication, your child will undergo baseline testing including a basic metabolic blood screening, an electroencephalogram (EEG), and neurologic examination. The study neurologist will verify the findings stated by your child’s PCP in the prescreening questionnaire and will make the final determination if it is safe for your child to be enrolled in the study. If it is determined safe for your child to continue in the study, several b
be administered by the department of neuropsychology on daay 2. The study coordinator will contact you via telephone throughout the study to give you a chance to ask questions or voice concerns regarding the study. The coordinator will also ask you questions regarding your child’s tolerance to the study drug, behavioral changes you may observe and verify adherence to the dosing regimen.
After 8 weeks of treatment, you and your child will be required to travel to the study site again. During this visit, your child will undergo an EEG, neurologic examination, behavioral testing and be asked to provide a blood sample. The testing will be administered over 2 days and
those performed during the baseline testing.
One month after the study medication has been started; the study coordinator will contact you via telephone and conduct a study interview. This interview will assess your child’s tolerance of the study drug and behavioral changes you may observe.
Finally 16 weeks after the first study visit, you and your child will be required to travel to the study site again. During this visit, your child will undergo an EEG, neurologic examination, behavioral testing and be asked to provide a blood sample. The testing will be administered over 2 days and will involve the same tests as those performed during the baseline testing.
IC Parental Permission Template – Med/SocBeh Rev: 2010-09-03
**You should continue to administer any medications your child was receiving at the time of
After you have read and then reviewed this informed consent form (ICF), a signed paper copy of the ICF will need to be returned to the study staff. Once the signed ICF has been received, you will be sent a prescreening questionnaire that must be completed by your child’s primary care physician (PCP
completed prescreening form should be returned directly from the PCP to the study coordinator. The prescreening questionnaire will help the study staff determine if it is safe for your child to participate in the study and if your child falls within the inclusion and exclusion criteria prior to traveling to the study site. You will be notified by telephone if your child has been selected to participate in the study.
Upon arrival to the study site and before your child receives study medication, your child will undergo baseline testing including a basic metabolic blood screening, an electroencephalogram (EEG), and neurologic examination. The study neurologist will verify the findings stated by your child’s PCP in the prescreening questionnaire and will make the final determination if it is safe for your child to be enrolled in the study. If it is determined safe for your child to continue in the study, several b
be administered by the department of neuropsychology on daay 2. The study coordinator will contact you via telephone throughout the study to give you a chance to ask questions or voice concerns regarding the study. The coordinator will also ask you questions regarding your child’s tolerance to the study drug, behavioral changes you may observe and verify adherence to the dosing regimen.
After 8 weeks of treatment, you and your child will be required to travel to the study site again. During this visit, your child will undergo an EEG, neurologic examination, behavioral testing and be asked to provide a blood sample. The testing will be administered over 2 days and
those performed during the baseline testing.
One month after the study medication has been started; the study coordinator will contact you via telephone and conduct a study interview. This interview will assess your child’s tolerance of the study drug and behavioral changes you may observe.
Finally 16 weeks after the first study visit, you and your child will be required to travel to the study site again. During this visit, your child will undergo an EEG, neurologic examination, behavioral testing and be asked to provide a blood sample. The testing will be administered over 2 days and will involve the same tests as those performed during the baseline testing.
IC Parental Permission Template – Med/SocBeh Rev: 2010-09-03
**You should continue to administer any medications your child was receiving at the time of