Tadalafil entfaltet seine Wirkung über eine selektive Hemmung der PDE5, wodurch die Konzentration von cGMP im glatten Muskelgewebe stabil bleibt. Diese biochemische Modulation resultiert in einer langanhaltenden Relaxation der Gefäßwände. Der Wirkstoff wird nach oraler Einnahme effizient resorbiert, mit einer Bioverfügbarkeit von rund 80 %. Seine Halbwertszeit von bis zu 36 Stunden ist innerhalb dieser Substanzklasse außergewöhnlich. Abgebaut wird er in der Leber, hauptsächlich durch CYP3A4, mit anschließender biliärer Exkretion. Typische unerwünschte Wirkungen entstehen durch eine verstärkte Vasodilatation, etwa Kopfschmerzen oder Flush. Pharmakologisch wird cialis generika vor allem durch die verlängerte Wirkungsdauer charakterisiert.
Asthma care in the emergency department
Approved 11/08 Division of Pediatric Emergency Medicine
Asthma Care in the Emergency Department Clinical Practice Guideline Inclusion: 1) Children 2 years of age or older with a prior history of wheezing, and 2) Children less than 2 years of age with likely Asthma rather than Acute Bronchiolitis Exclusion: History of unstable heart disease or suspicion of other reason for wheezing (laryngomalacia, tracheomalacia, foreign body, etc.) Time 0: Obtain vital signs, pulse oximetry and height in children older than 6 years, then determine initial asthma score: Modified CAS (Woods and Downes) Asthma Score: Initial Asthma Score CAS 02 CAS 3 CAS 510
Continuous Albuterol with Atroventneb over
Approved 11/08 Division of Pediatric Emergency Medicine
Repeat Asthma Score at 1 hour CAS 12 CAS 3 CAS 510
Continuous Albuterolneb over 1 hour. Repeat Asthma Score at 2 hours CAS 12 CAS 3 CAS 510
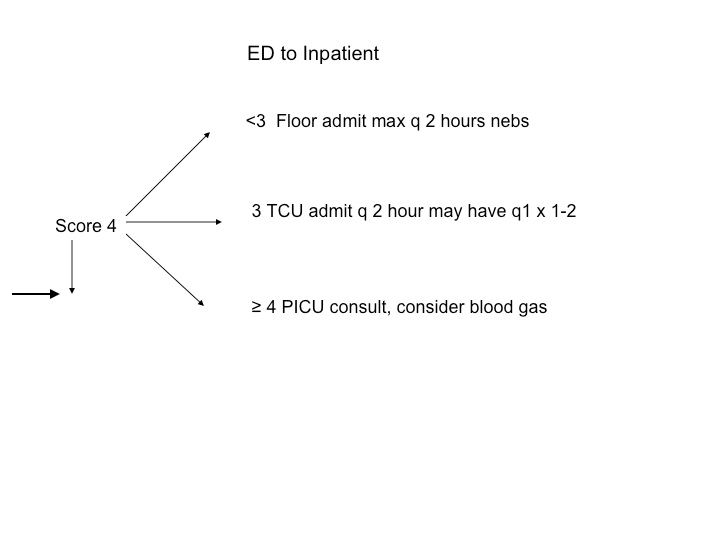
Continuous Albuterol neb over 1 hour. Repeat Asthma Score at 3 hour CAS 12 CAS 3 CAS 410 Admit to Floor Admit to TCU Admit PICU.
q 2 hour nebs. May have q 1hour x 1‐2
Approved 11/08 Division of Pediatric Emergency Medicine
Nebulization Dosing Wt > 20 kg Wt < 20 kg Score 0 – 2
Oral steroids 2mg/kg 2 mg/kg up to 60 mg
Approved 11/08 Division of Pediatric Emergency Medicine
Cardinal Glennon Children’s Medical Center Asthma Care in the Emergency Department
Asthma is a major public health problem of increasing concern in the United States. From 1980 to 1996, asthma prevalence among children increased by an average of 4.3% per year, from 3.6% to 6.2%. Low-income populations, minorities, and children living in inner cities experience disproportionately higher morbidity and mortality due to asthma. Asthma’s effects on children and adolescents include the following:
• Asthma accounts for 14 million lost days of school missed annually.
• Asthma is the third-ranking cause of hospitalization among those younger than
• The number of children dying from asthma increased almost threefold from 93 in
• The estimated cost of treating asthma in those younger than 18 years of age is
The pathophysiology of asthma is composed of:
‐ Bronchoconstriction by bronchial smooth muscle contraction
Emergency department management of asthma includes:
‐ Oxygen to maintain pulse oximetry>90%
‐ Short acting beta agonist therapy in the form of repetitive or continuous
administration: three treatments spaced every 20-30 minutes or continuous administration
‐ Inhaled ipratropium bromide particularly for patients with severe airflow
‐ Corticosteroids by the parenteral or oral routes
‐ Intravenous magnesium sulfate and beta agonists (terbutaline)
Approved 11/08 Division of Pediatric Emergency Medicine
Unproven Therapy:
(theophylline/amiophylline) is not recommended though it may
be utilized as an aggressive measure to stave off intubation
Emergency Department Asthma Care Pathway Who Qualifies:
1) Children older than 2 years of age with a prior history of wheezing, and 2) Children less than 2 years of age with likely asthma rather than acute bronchiolitis
Who Does NOT Qualify:
Children with unstable heart disease or suspicion of other reasons for wheezing, such as a laryngomalacia, tracheomalacia, or foreign body
Step 1: Obtain vital signs, pulse oximetry and height in children older than 6 years. Step 2: Determine asthma score: Modified CAS (Woods and Downes) Asthma Score. Asthma score < 3
1 - Order a single albuterol nebulizer treatment of 5 mg for children weighing
20 kg. and above, or 2.5 mg for children less than 20 kg.
3 – The RN should initiate the treatment if respiratory therapy has not arrived
Approved 11/08 Division of Pediatric Emergency Medicine
Asthma score 3 to 5
1 - Place the child on continuous pulse oximetry
2 - Order a continuous nebulization treatment with albuterol and atrovent to
Run over 1 hour: 10 mg and 250 micrograms in children less than 20 kg.
20 mg and 500 micrograms in children 20 kg and above.
The RN should initiate the treatment if respiratory therapy has not
3 – Request the respiratory therapy check post treatment peak flows in
4 – Order and administer 2 mg/kg of oral steroid (form at the discretion of
the RN) with a maximum of 60 mg. Notify MD if unable to tolerate PO
5 – Place the chart in the door, notify the attending or fellow of patient’s
enrollment in the pathway and when the nebulization treatment is
Asthma score > 5
1 – Place the child on continuous pulse oximetry
2 – The RN initiates a continuous nebulization treatment if respiratory
3 – Notify the attending or fellow of patient’s enrollment and need for their
4 - The timing and route of administration of steroids as well as any
supplemental medications (Magnesium, terbutaline, etc.) should
be determined by the attending or fellow at the time of their evaluation.
Magnesium: 25 - 75 mg/kg IV up to 2 grams Therbutaline: 2 – 10 mcg/kg IV load followed by 0.1 – 0.4 mcg/kg/min.
(May titrate in incements of 0.1 – 0.2 mcg/kg/min Q 30 min)
Approved 11/08 Division of Pediatric Emergency Medicine
Admission of asthma patients:
The pathway for admission of patients to the appropriate unit in the hospital
is outlined in the ED to Inpatient Admission Pathway.
Discharge from the emergency department requires that:
‐ If the patient is able to perform an appropriate peak flow it should be greater than
or equal to 70% of predicted (available in table format with peak flow meters)
‐ The patient is comfortable and is able to tolerate oral meds and fluids as well as
‐ The above conditions remain stable 30 to 60 minutes after the last nebulized
Discharge medications:
‐ Inhaled bronchodilator (albuterol via a home nebulizer or MDI) including
education in the use of an MDI as indicated. Albuterol: MDI: 2 – 4 puffs, Nebulizer: 2.5 mg.
‐ Oral corticosteroids (2 mg/kg/day, max. of 60 to 80 mg) for 4 to 5 days
‐ Continuation of any current asthma medications (long term bronchodilators,
‐ Consider adding an inhaled corticosteroid for patients with persistent disease
‐ Follow-up with a health care provider in 1 week
Approved 11/08 Division of Pediatric Emergency Medicine
Internationale Blumenkoordination (IFC) Richtlinien für die sozial- und umweltverträgliche Produktion von Schnittblumen, Farn, Pflanzen und Füllgrün Die internationale Blumenkoordination unterstützt den sozial- und umweltverträglichen An-bau von Blumen, Farn, Pflanzen und Füllgrün sowohl in den Ländern des Südens wie auch des Nordens, indem sie einheitliche Standards setzt.
Zusammenstellung der fachlichen praktischen, publizistischen und wissenschaftlichen Aktivitäten von Dr. med. Armin Aeschbach Dr. med. Armin Aeschbach, Facharzt Anästhesie Intensivmedizin FMH, Schmerztherapie - Dozent/Ausbildner von Assistenten und Fachärzten in Interventioneller Schmerztherapie - Dozent an praktischen schmerzinterventionellen Workshops/Kursen - Publikationen in Fac
 Approved 11/08 Division of Pediatric Emergency Medicine
Asthma Care in the Emergency Department
Approved 11/08 Division of Pediatric Emergency Medicine
Asthma Care in the Emergency Department 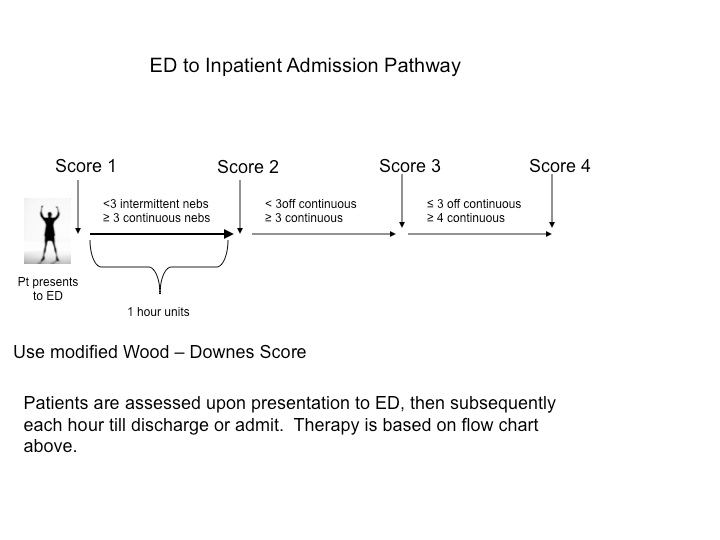
 Approved 11/08 Division of Pediatric Emergency Medicine
Approved 11/08 Division of Pediatric Emergency Medicine