Tadalafil entfaltet seine Wirkung über eine selektive Hemmung der PDE5, wodurch die Konzentration von cGMP im glatten Muskelgewebe stabil bleibt. Diese biochemische Modulation resultiert in einer langanhaltenden Relaxation der Gefäßwände. Der Wirkstoff wird nach oraler Einnahme effizient resorbiert, mit einer Bioverfügbarkeit von rund 80 %. Seine Halbwertszeit von bis zu 36 Stunden ist innerhalb dieser Substanzklasse außergewöhnlich. Abgebaut wird er in der Leber, hauptsächlich durch CYP3A4, mit anschließender biliärer Exkretion. Typische unerwünschte Wirkungen entstehen durch eine verstärkte Vasodilatation, etwa Kopfschmerzen oder Flush. Pharmakologisch wird cialis generika vor allem durch die verlängerte Wirkungsdauer charakterisiert.
491.pmd
PCI in Hyperkalemia Case Report Primary PCI in a Patient of Inferior ST-segment Elevation Myocardial Infarction in the Time of Severe Hyperkalemia: A Case Report. Deepak Natarajan, Chiranjib Deb, Vijeta Maheshwari,Mafooza Rashid, Betsheba Dinaker, Nirmalya Mukherjee. Department of Interventional Cardiology, Moolchand MedCity, New Delhi.Abstract This case report describes the management of a middle-aged hypertensive male patient who presented with acute inferior ST-segment elevation myocardial infarction accompanied with severe hyperkalemia. His coronary angiography revealed a thread like right coronary artery along its entire course and normal left coronary artery system with patent coronary stents in the left anterior descending and left circumflex arteries. Subsequent to correction of hyperkalemia with intravenous calcium gluconate and regular insulin the patient underwent primary percutaneous coronary intervention (PPCI)of the right coronary artery with the deployment of a sirolimus eluting stent. The patient received overnight an infusion of tirofiban at half the usual dose between the diagnostic coronary angiogram and PPCI. Key Words : Hyperkalemia, ST-segment elevation myocardial infarction, calcium gluconate, primary percutaneous coronary intervention, regular insulin. INTRODUCTION
Severe hyperkalemia defined as serum potassium level greaterthan 6.5 mEq/L albeit not uncommon is a life threatening conditionthat if not treated immediately can be catastrophic. We describethe management of a middle aged male patient who presentedwith acute inferior ST-segment elevation myocardial infarctionaccompanied by severe hyperkalemia. CASE REPORT
A 63 year old hypertensive male was admitted for severe
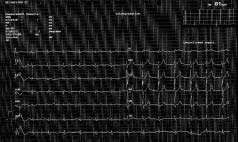
Figure 1: Peaking of T waves from V2 to V5 and absence of P waves.
intermittent retrosternal chest pain for the previous 10 hours. Hehad underwent percutaneous coronary intervention (PCI) 4
A diagnosis of acute inferior ST elevation myocardial infarction
years ago when 2 bare metal stents had been deployed in mid left
(STEMI) with right ventricle infarction was made. Two litres of
anterior descending (LAD) and left circumflex (LCX) arteries. He
normal saline were rapidly infused intravenously and after an
had been on 75 mgm of aspirin, 5 mgm of ramipril, sustained
informed consent the patient was shifted to the catheterization
release 25 mgm metoprolol and 10 mgm of atorvostatin. He had
laboratory for primary PCI. His coronary angiogram done from
however resumed smoking more than 15 cigarettes a day. He had
the right femoral route showed patent stents in the LAD and LCX
on this occasion consumed more than a couple of diclofenac
arteries with no significant lesions in the left coronary system
tablets at his chest pain onset. On admission to the ER he
( figure 2). The right coronary artery ( RCA) however was thread
appeared disoriented and agitated, had a heart rate of 35 to 40
like in appearance . There was no change in the caliber of the RCA
per minute, systolic blood pressure of 70 mm Hg and had 86%
following 2 (50 mcg) boluses of intracoronary nitroglycerin (
oxygen saturation breathing room air. There were basal
crepitations while his respiration was 28 to 30 per minute. His 12
His laboratory investigations showed hemoglobin 12 gm %, total
lead ECG revealed a sinus rate of 38 per minute, significant ST
leukocytes 11,000 per cc, and platelets of 160,000 per cc. He had
segment elevation in L2,L3 and AVF with ST segment depression
random sugar of 110 mgm % , blood urea 60 mgm %, serum
in the precordial leads. There was also suggestion of peaking of
creatinine 2.2 mgm %, serum potassium of 7.8 mEq/L, sodium 142
T waves from V2 to V5 and absence of P waves ( figure 1). The
mEq/L and severe metabolic acidosos ( pH 7.20, CO2 46 mmHg,
2D echocardiogram demonstrated a normal sized left venticle
O2 82 mmHg, HCO3 -18 mEq/L, lactic acid 2.50 mEq/L). The CPK
with akinesia of the inferior wall and an ejection fraction of 50%.
was 1715 units and CPK-MB was 102 units. Correspondence: Dr. Deepak Natarajan, Department of Interventional Cardiology, Moolchand MedCity, New Delhi. E-mail: deepaknatarajan19@gmail.com Natarajan et al. Figure 2: Patent stents in the Figure 3: The right coronary Figures 5-6: Brisk antegrade TIMI 3 flow was achieved with no residual
The hyperkalemia was immediately treated with intravenous 10ml of 10% calcium gluconate, 10 units of regular insulin in 100 mlof 50% dextrose intravenously and 50 mmol of intravenoussodium bicarbonate. This regimen was repeated twice more at 6hour intervals. In view of the severe hypekalemia it was decided to correct theelectrolyte imbalance first and then proceed to PCI. The patientwas given a bolus of 15 mcg/Kg of tirofiban followed by aninfusion of (0.075 mcg/Kg/ minute) for 10 hours. The next morning subsequent to positioning a temporary pacinglead in the right ventricle apex his RCA injection revealed a criticaltight 90% proximal ulcerated stenosis (figure 4). His potassium
Figure 7: ECG on discharge exhibited sinus rhythm with fully resolved ST segment resolution and small Q waves in the inferior leads, without
had normalized to 4.1 mEq/L while his creatinine was 2.1
mgm%.The RCA was engaged by a 6 Fr JR guiding catheter and
DISCUSSION
a 0.014 inch floppy wire was negotiated across the block. A 2.25X 16 mm sirolimus stent was deployed at 16 atm subsequent to
This report describes the management of a patient with an acute
predilatation with a 1.5 X 10 mm balloon. Brisk antegrade TIMI
inferior STEMI accompanied by severe hyperkalemia. Severe
3 flow was achieved with no residual stenosis ( Figures 5-6).
hyperkalemia ( potassium more than 7.5 mEq/L) if left untreated
The patient was kept on ion exchange resins till discharge along
carries a high mortality of more than 65%. It is imperative that
with dual antiplatelet and statin thereapy.At discharge the
hyperkalemia presenting with electrocadiographic changes or
potassium was 4.3 mEq/L, sodium 135 mEq/L, blood urea 61
more than 6.5 mEq/L is rapidly corrected 1-4.
mgm% and serum creatinine 1.8 mgm%. The ECG on discharge
However in almost 50% of patients with serum potassium more
exhibited sinus rhythm with fully resolved ST segment resolution
than 6.5 mEq/L there may be no electrocardiographic changes5.The
and small Q waves in the inferior leads, without evidence of
other point to bear in mind for the clinician is that more than 60%
hyperkalemia. Segment resolution and small Q waves in the
patients presenting with severe hyperkalemia have an underlying
inferior leads, without evidence of hyperkalemia ( Figure 7).
renal impairment or have been on a single or a cocktail ofpotassium retaining medication. The earliest ECG change observed with hyperkalemia are anabsence of P wave, peaking and narrowing of T wave andshortening of the corrected QT interval. In cases of severehyperkalemia other ECG manifestations seen are left and rightbundle branch like widening of QRS complexes that can bedistinguished from genuine bundle bundle branch block by thefact that in the latter the conduction delay is in the middle or thefinal stage whereas in hyperkalemia the widening is diffuse. Inthe final stages there is merging of the QRS complex and T waveproducing a sinusoidal wave with QT interval prolongation . Insome patients ST -segment elevation and depression can also
Figure 4: RCA revealed a critical tight 90% proximal ulcerated stenosis. PCI in Hyperkalemia
be seen mimicking an acute myocardial infarction. This is known
and eptifibatide can both be given as usual boluses but the
as a “ dialyzable injury current” 6-8.
infusion rate will need to be halved. Eptifibatide is contraindicated
Emergency treatment for severe hyperkalemia should be initiated
immediately with intravenous infusion of calcium gluconate that
A tight almost ulcerated subtotal occlusion of the RCA was seen
begins to stabilizes the myocardial cell within 2-3 minutes but
the following morning subsequent to 10 hours tirofiban ( half
acts for only 30 to 60 minutes. Calcium chloride can also be used
dose) infusion and this was easily treated by percutaneous
but as it is three times potent than calcium gluconate the dose
intervention deploying a sirolimus stent. The patient was
has to be reduced. Calcium stabilizes the cell by maintaining the
subsequently managed on aspirin, clopidogrel, and atorvastatin.
15 mV gap between the resting membrane and threshold potentials. The normal resting membrane potential is made less negative
CONCLUSION
from -90 mV to -80 mV. This is closer to the threshold potential
This report underscores the fact that a patient presenting with
of -75 mV and thereby makes it more vulnerable to lethal tachy-
acute STEMI accompanied with severe hyperkalemia requires
arrhythmias. Calcium may also speed up impulse formation in the
immediate treatment of the raised potassium levels with calcium
sinoatrial and atrioventricular nodal cells reversing myocardial
(because of its rapid stabilization of the myocardial cell) followed
depression seen with hyperkalemia 9-10.
by insulin with or without glucose. Ion exchange resins are
Serum potassium is next reduced with 10 units of regular insulin
employed next to continue reducing serum potassium.
given intravenously.Insulin drives the excess potassium into
Percutaneous coronary intervention is safe and effective
the intracellular space by stimulating the Na-K ATPase pump in
subsequent to normalization of potassium serum levels.
exchange with sodium in a 2:3 ratio. This effect is independent
Adjunctive GPI’s can be used with careful monitoring of dosage
of glucose Therefore if a patient is already hyperglycemic extra
dextrose need not be administered. Insulin begins to act in 30 to60 minutes and reduces potassium by 0.5 to 1.0 mEq/L 11. REFERENCES
Nebulized salbutamol in high doses of 10 mgm has also been
1. Acker CG, Johnson JP, Palevsky PM,Greenberg A. Hyperkalemia in hospitalized
shown to reduce potassium levels by 0.62 to 0.98 mEq/L. patients: causes,adequacy of treatment, and results of an attempt to improve physician
Salbutomal has been seen to be safe and effective. It is therefore
compliance with published therapy guidelines. Arch Intern Med 1998;158:917-24.
recommended to be employed as adjunctive treatment for patients
2. Greenberg A. Hyperkalemia: treatment options. Semin Nephrol 1998;18:46-57. 3. Weisberg LS. Management of severe hyperkalemia. Crit Care Med 2008; 36:3246-51.
with severe hyperkalemia. Sodium bicarbonate albeit capable of
4. Nyirenda MJ, Tang JI, Padfield PL, Seckl JR. Hyperkalemia. BMJ 2009; 339:1019-24.
shifting potassium from extracellular to intracellular space by
5. Szerlip HM, Weiss J, Singer I.Profound hyperkalemia without electrocardiographic
increasing blood pH is not recommended for routine usage
disturbances. Am J Kidney Dis 1986;7:461-5.6. Mattu A, Brady WJ, Robinson DA. Electrocardiographic manifestations of
because the effect is little and short lasting 12-13. hyperkalemia. Am J Emerg Med 2000;18:721-9.
In the event of persisting hyperkalemia the quickest technique
7. Montague BT, Oullette JR, Buller GK. Retrospective review of the frequency of ECG
is to use hemodialysis. It is however rarely utilized because of its
changes in hyperkalemia. Clin J Am Soc nephrol 2008; 3: 324-30.
expense and invasive nature. The usual substitute is orally or
8. Zaikas A, Basagiannis C, Stiliadis I. Psuodoinfarction pattern in a patient withhyperkalemia, diabetic ketoacidosis and normal coronary vessels: A case report. J
rectally administered ion exchange resins that exchange
potassium for sodium ions. Exchange resins decrease serum
9. Winkler AW, Hoff HE, Smith PK. Factors affecting the toxicity of potassium. Am J
potassium by about 1 mEq/L in 24 hours. 10. Beeler GW, Reuter H. Membrane calcium current in ventricular myocardial fibres. J
This patient was on an angiotensin converting inhibitor, a long
acting beta blocker, and upon that had consumed more than a
11. Blumberg A, Weidmann P, Shaw S, Gnadinger M. Effect of various therapeutic
couple diclofenac tablets. It is quite probable that these 3 drugs
approaches on plasma potassium and major regulating factors in terminal renal
tilted the serum potassium to a dangerous level in this patient
12. Blumberg A, Weidmann P, Ferrari P. Effect of prolonged bicarbonate administration
who also had impaired kidney function as suggested by his
on plasma potassium in terminal renal failure. Kidney Int 1992; 41:369-74.13. Allon M. Copkney C. Albuterol and insulin for treatment of hyperkalemia in
Percutaneous intervention was deferred in view of the severe
Hemodialysis patients. Kidney Int 1990;38:869-72.14. Alexander KP, Chen AY, Roe MT,et al., for the CRUSADE Investigators. Excess dosing
hyperkalemia and the fact that the RCA initially despite
of antiplatelet and antithrombin agents in the treatment of non ST segment elevation
intracoronary injections of nitroglycerine remained thread like. acute coronary syndromes. JAMA 2005;294:3108-16.
It may be hypothesized that in the setting of severe hyperkalemia
15. Tsai TT, Maddox TM, Roe MT, et al., for the National Cardiovascular Data Registry.
the infarct related vessel goes into diffuse vaso-spasm. Contraindicated medication use in dialysis patients undergoing percutaneous coronaryinterventions. JAMA 2009; 302:2458-64.
Abciximab is the safest glycoprotein 2b/3a inhibitor( GPI) that
16. Best PJ, Lennon R, Gersh BJ, et al. Safety of abciximab in patients with chronic renal
can be administered in patients with significantly impaired
insufficiency who are undergoing percutaneous coronary interventions. Am Heart J
glomerular filtration without any alteration in dosage. Tirofiban
L’AUTORITÀ GARANTE DELLA CONCORRENZA E DEL MERCATO NELLA SUA ADUNANZA del 14 dicembre 2011; SENTITO il Relatore Dottor Salvatore Rebecchini; VISTA la Parte II, Titolo III, del Decreto Legislativo 6 settembre 2005, n. 206, recante “ Codice del Consumo ” e successive modificazioni (di seguito, Codice del Consumo); VISTO il “ Regolamento sulle procedure istruttorie in materia di prat
Ibrahim Ethem Bagci1, Mohammad Reza Pourmirza1, Shahid Raza2, Utz Roedig1, Thiemo Voigt2,31School of Computing and Communications, Lancaster University, Lancaster, UK{i.bagci, m.pourmirza, u.roedig}@lancaster.ac.uk2Swedish Institute of Computer Science, Kista, SwedenAbstract—Many Wireless Sensor Networks (WSNs) are used toTo secure data stored on nodes it has been proposed tocollect and pr

 PCI in Hyperkalemia
PCI in Hyperkalemia




 Natarajan et al.
Natarajan et al. PCI in Hyperkalemia
PCI in Hyperkalemia