Tadalafil entfaltet seine Wirkung über eine selektive Hemmung der PDE5, wodurch die Konzentration von cGMP im glatten Muskelgewebe stabil bleibt. Diese biochemische Modulation resultiert in einer langanhaltenden Relaxation der Gefäßwände. Der Wirkstoff wird nach oraler Einnahme effizient resorbiert, mit einer Bioverfügbarkeit von rund 80 %. Seine Halbwertszeit von bis zu 36 Stunden ist innerhalb dieser Substanzklasse außergewöhnlich. Abgebaut wird er in der Leber, hauptsächlich durch CYP3A4, mit anschließender biliärer Exkretion. Typische unerwünschte Wirkungen entstehen durch eine verstärkte Vasodilatation, etwa Kopfschmerzen oder Flush. Pharmakologisch wird cialis generika vor allem durch die verlängerte Wirkungsdauer charakterisiert.
Ica summative
FACULTY OF MEDICINE UNIVERSITY OF SYDNEY MEDICAL PROGRAM YEAR 3
MED 3 SUMMATIVE MEQ PAPER 1 QUESTION COPY
Thomas Werner is a 50 year old man with insulin requiring Type 2 diabetes who presents to the Emergency Department with severe left loin pain and high fevers of 24 hours duration. He looks very unwell and his temperature is 39°C. His blood pressure is 80/50 mmHg and his heart rate is 120/min. His diabetes is normally well controlled. The glucometer reading on presentation is *19.5 mmol/L (NR 3.0-7.7 mmol/L). Dipstick urinalysis is positive for blood, leucocytes, protein, glucose and nitrites.
1. What is your diagnostic hypothesis?
2. Briefly describe the pathophysiological mechanisms that account for: a) Mr Werner’s clinical presentation including b) Mr Werner’s elevated blood sugar level.
Suggested Time = 12 min Questions 1 & 2 of 6 Cumulative Time = 12 min
Thomas Werner is a 50 year old man with insulin requiring Type 2 diabetes who presents to the Emergency Department with severe left loin pain and high fevers of 24 hours duration. He looks very unwell and his temperature is 39°C. His blood pressure is 80/50 mmHg and his heart rate is 120/min. His diabetes is normally well controlled. The glucometer reading on presentation is *19.5 mmol/L (NR 3.0-7.7 mmol/L). Dipstick urinalysis is positive for blood, leucocytes, protein, glucose and nitrites. You suspect that Mr Werner has pyelonephritis resulting in septic shock and elevation of his blood sugar level. You organise a septic work-up and serum biochemistry, and book Mr Werner for an urgent abdominal X-ray and CT scan. 3. Describe your initial management plan. State the underlying aims for each component of your management strategy.
Suggested Time = 6 min Question 3 of 6 Cumulative Time = 18 min
Thomas Werner is a 50 year old man with insulin requiring Type 2 diabetes who presents with severe left loin pain and high fevers of 24 hours duration. He looks very unwell and his temperature is 39°C. His blood pressure is 80/50 mmHg and his heart rate is 120/min. Dipstick urinalysis is positive for blood, leucocytes, protein, glucose and nitrites. The glucometer reading on presentation is *19.5 mmol/L (NR 3.0-7.7 mmol/L). You suspect that Mr Werner has pyelonephritis resulting in septic shock and elevation of his blood sugar level. You have organised a septic workup. Mr Werneris treated with intravenous fluids, antibiotics and insulin. His blood pressure improves to 105/75 mmHg but his pulse remains at 120/min. His blood glucose is now *10.2 mmol/L. An abdominal X-ray suggests the presence of a 20x10 millimetre poorly opacified density in the region of the kidney. The left kidney is found on non-contrast CT to be grossly hydronephrotic and obstructed at the pelvi-ureteric junction by a large calculus. The fluid in the renal pelvis is of higher density than water.
4. Mr Werner has no known allergies. What antibiotic/s should he receive? Justify your choice/s.
5. When and how should the obstruction be managed?
Suggested Time = 9 min Questions 4 & 5 of 6 Cumulative Time = 27 min
Thomas Werner is a 50 year old man with insulin requiring Type 2 diabetes who presents with severe left loin pain and high fevers of 24 hours duration. You suspect that Mr Werner has pyelonephritis resulting in septic shock and elevation of his blood sugar level. Mr Werner is treated with intravenous fluids and insulin. His blood pressure improves to 105/75 mmHg and his blood glucose is now *10.2 mmol/L. Over the next few days Mr Werner improves with further treatment. Mr Werner tells you that he has recently been in prison for six months on a fraud-related charge. He has only been out of prison for a month or so and is back living with his wife and two children. 6. List 2 ways in which prison inmates may contribute to the burden of illness on their return to the general community?
Suggested Time = 4 min Question 6 of 6 Cumulative Time = 31 min
END OF CASE 1
A comatose 25 year old woman is brought into the Emergency Department by ambulance. It is 23:00 on a busy Saturday night and you are the resident medical officer on duty. The ambulance officer says she has taken an overdose of alcohol and tablets.
1. Describe the initial steps (first 5-10 minutes) you will take to assess this patient?
Suggested Time = 5 min Question 1 of 7 Cumulative Time = 36 min
A comatose 25 year old woman is brought into the Emergency Department by ambulance. It is 23:00 on a busy Saturday night and you are the resident medical officer on duty. The ambulance officer says she has taken an overdose of alcohol and tablets. The woman is mumbling incomprehensibly. You perform a quick primary survey of her condition. Her airway is patent, her gag reflex is intact and her respiratory pattern appears normal. Her pupils are midsize and reactive to light. Her oxygen saturation is 92% on room air (NR 95-98%), her heart rate is 109 and regular, her BP is 85/70, and body temperature is 36.9°C. Her blood glucose is 7.0mmol/L (NR 3.0-7.7 mmol/L). Her peripheries are well perfused.
2. What urgent management is required at this initial stage to address these clinical findings?
3. What further history is required and how would you acquire it?
Suggested Time = 10 min Questions 2 & 3 of 7 Cumulative Time = 46 min
A comatose 25 year old woman is brought into the Emergency Department by ambulance. It is 23:00 on a busy Saturday night and you are the resident medical officer on duty. The ambulance officer says she has taken an overdose of alcohol and tablets. She mumbles incomprehensibly. You perform a quick primary survey of her condition. Her airway is patent, her gag reflex is intact and her respiratory pattern appears normal. Her pupils are midsize and reactive to light. Her oxygen saturation is 93% on room air (NR 95-98%), her heart rate is 109 and regular, her BP is 85/70, and body temperature is 36.9°C. Her blood glucose is 7.0mmol/L. Her peripheries are well perfused. The ambulance officer has brought in a number of empty drug strips, and says he brought all the drug packaging that they could find at the woman’s home. The woman’s boyfriend had called the ambulance at 21:30 hours. He said that his girlfriend had disappeared into the bedroom for a short while after they had an argument. She then returned to the living room and told him “I’ve just taken some tablets”. Earlier that evening, he and his girlfriend had finished three bottles of wine. The empty strips include: 20 X 10mg temazepam and 26 X 500mg paracetamol. The local doctor had prescribed the temazepam for “difficulty sleeping”. There are no further details of the medical or psychiatric history available. Following treatment, her BP improves to 110/70 and her oxygen saturation is now 98%. Her Glasgow Coma Score is 11 (opens eyes to voice=3; mumbles incomprehensible sounds=2; and can obey simple motor commands=6). Her pupils are midsize and reactive to light. There are no focal neurological signs, and no signs of external injury. There are no track marks. Chest and abdominal examinations are normal.
4. How would you investigate and manage this patient now?
Suggested Time = 6 min Question 4 of 7 Cumulative Time = 52 min
A comatose 25 year old woman is brought into the Emergency Department by ambulance. It is 23:00 on a busy Saturday night. The ambulance officer says she has taken an overdose of alcohol and tablets. You perform a quick primary survey of her condition. Her airway is patent, her gag reflex is intact and her respiratory pattern appears normal. She mumbles incomprehensibly and obeys simple motor commands. Her pupils are midsize and reactive to light. Her oxygen saturation is 93% on room air (NR 95-98%), her heart rate is 109 and regular, her BP is 85/70, and body temperature is 36.9°C. Her blood glucose is 7.0mmol/L. Her peripheries are well perfused. The ambulance officer has brought in a number of empty drug strips, and says he brought all the drug packaging that they could find at the woman’s home. The woman’s boyfriend had called the ambulance at 21:30 hours. He said that his girlfriend had disappeared into the bedroom for a short while after they had an argument. She then returned to the living room and told him “I’ve just taken some tablets”. Earlier that evening, he and his girlfriend had finished three bottles of wine. The empty strips include: 20 X 10mg temazepam and 26 X 500mg paracetamol. The local doctor had prescribed the temazepam for “difficulty sleeping”. There are no further details of the medical or psychiatric history available. Following treatment, her BP improves to 110/70 and her oxygen saturation is now 98%. Her Glasgow Coma Score is 11 (opens eyes to voice=3; mumbles incomprehensible sounds=2; and can obey simple motor commands=6). Her pupils are midsize and reactive to light. There are no focal neurological signs, and no signs of external injury. There are no track marks. Chest and abdominal examinations are normal. Her paracetamol level taken at 4 hours post-ingestion is 1450 µmol/l and the nomogram is on the opposite page.
5. What do you do now? Justify your answer.
Suggested Time = 5 min Question 5 of 7 Cumulative Time = 57 min Nomogram
A comatose 25 year old woman is brought into the Emergency Department by ambulance. It is 23:00 on a busy Saturday night. The ambulance officer says she has taken an overdose of alcohol and tablets. The ambulance officer has brought in a number of empty drug strips, and says he brought all the drug packaging that they could find at the woman’s home. The woman’s boyfriend had called the ambulance at 21:30 hours. He said that his girlfriend had disappeared into the bedroom for a short while after they had an argument. She then returned to the living room and told him “I’ve just taken some tablets”. Earlier that evening, he and his girlfriend had finished three bottles of wine. The empty strips include: 20 X 10mg temazepam 26 X 500mg paracetamol. The local doctor had prescribed the temazepam for “difficulty sleeping”. There are no further details of the medical or psychiatric history available. Her paracetamol level taken at 4 hours post-ingestion is 1450µmol/l. Eight hours later the patient, Michelle Gould, has woken up and wants to go home. She is willing to sign a “discharge at own risk” form. Her boyfriend has left the Emergency Department telling you and Michelle that he doesn’t want anything more to do with her. You find out that she has no home of her own and so now has nowhere to live. Michelle hasn’t had contact with her family for several years as she left home when she was sixteen and has spent a lot of time living on the streets.
6. Homelessness has been described as a spectrum of living conditions from total lack of shelter through to poor quality rooming house accommodation. Describe in a short paragraph the demographic and health features of homeless people in Australia. (Provide 6 features)
Suggested Time = 8 min Question 6 of 7 Cumulative Time = 65 min
A comatose 25 year old woman is brought into the Emergency Department by ambulance. It is 23:00 on a busy Saturday night. The ambulance officer says she has taken an overdose of alcohol and tablets. The ambulance officer has brought in a number of empty drug strips, and says he brought all the drug packaging that they could find at the woman’s home. The woman’s boyfriend had called the ambulance at 21:30 hours. He said that his girlfriend had disappeared into the bedroom for a short while after they had an argument. She then returned to the living room and told him “I’ve just taken some tablets”. Earlier that evening, he and his girlfriend had finished three bottles of wine. The empty strips include: 20 X 10mg temazepam 26 X 500mg paracetamol. The local doctor had prescribed the temazepam for “difficulty sleeping”. There are no further details of the medical or psychiatric history available. Her paracetamol level taken at 4 hours post-ingestion is 1450µmol/l. Eight hours later the patient, Michelle Gould, has woken up and wants to go home. She is willing to sign a “discharge at own risk” form. Her boyfriend has left the Emergency Department telling you and Michelle that he doesn’t want anything more to do with her. You find out that she has no home of her own and so now has nowhere to live. Michelle hasn’t had contact with her family for several years as she left home when she was sixteen and has spent a lot of time living on the streets.
7. When the psychiatric team confirms that Michelle is fit for discharge into the community, what accommodation options are available for her in Sydney? Provide 4 options.
Suggested Time = 5 min Question 7 of 7 Cumulative Time = 70 min
END OF CASE 2 Case 3
Andrew Jones is a 40 year old computer technician who in the past 6 months has been complaining of worsening left calf pain after walking 50 metres. He is unable to walk up hills and can only walk up steps slowly. He has also of late noted altered sensation to both feet not associated with ambulation. He has not seen a doctor for the past 10 years. He smokes 50 cigarettes per day and has done so for the last 15-20 years. His alcohol intake is 100g/day.
1. Provide at least two hypotheses that would explain Mr Jones’ presenting symptoms.
Suggested Time = 5 min Question 1 of 7 Cumulative Time = 75 min
Andrew Jones is a 40 year old computer technician who in the past 6 months has been complaining of worsening left calf pain after walking 50 metres. He is unable to walk up hills and can only walk up steps slowly. He has also of late noted altered sensation to both feet not associated with ambulation. He has not seen a doctor for the past 10 years. He smokes 50 cigarettes per day and has done so for the last 15-20 years. His alcohol intake is 100g/day. On physical examination the relevant findings are: weight 125 kg, height 180 cm, pulse rate 80 per minute, blood pressure 170/120 mmHg. Abdominal examination is normal. Upper limb pulses are normal. There are altered sensory changes to both feet and lower limb pulses are as follows: Lower limb pulses
2. Develop a problem list for this patient.
3. What initial investigations would you advise to further evaluate Mr Jones’ problems? Explain how each of the investigations you have selected helps you.
Suggested Time = 10 min Questions 2 & 3 of 7 Cumulative Time = 85 min
Andrew Jones is a 40 year old computer technician who in the past 6 months has been complaining of worsening left calf pain after walking 50 metres. He is unable to walk up hills and can only walk up steps slowly. He has also of late noted altered sensation to both feet not associated with ambulation. He has not seen a doctor for the past 10 years. He smokes 50 cigarettes per day and has done so for the last 15-20 years. His alcohol intake is 100g/day. On physical examination the relevant findings are: weight 125 kg, height 180 cm, pulse rate 80 per minute, blood pressure 170/120 mmHg. Abdominal examination is normal. Upper limb pulses are normal. Femoral pulses are both normal however the more peripheral lower limb pulses are reduced on the right and absent on the left. There are altered sensory changes to both feet. Results of further investigations are given in the table opposite. BP on this visit is 170/120 mmHg. 4.a) Reformulate your problem list for Mr Jones. b) Develop a comprehensive management plan for Mr Jones. (Provide management strategies, not details or specific pharmacological agents).
Suggested Time = 12 min Question 4 of 7 Cumulative Time = 97 min Investigations Mr Jones’ results Normal Range Full Blood Count Haemoglobin Biochemistry Sodium Other Investigations Urinary protein
ABI: There was a significant drop in ABI on treadmill exercise testing in the left leg and a mild fall in the right leg. The exercise test was terminated after one minute because of severe left calf pain. Left peripheral arterial scan demonstrated an occluded left superficial femoral artery with collateral flow into a patent popliteal artery.
Andrew Jones is a 40 year old computer technician who in the past 6 months has been complaining of worsening left calf pain after walking 50 metres. He is unable to walk up hills and can only walk up steps slowly. He has also of late noted altered sensation to both feet not associated with ambulation. He has not seen a doctor for the past 10 years. He smokes 50 cigarettes per day and has done so for the last 15-20 years. His alcohol intake is 100g/day. His weight is 125 kg, height 180 cm, pulse rate 80 per minute, blood pressure 170/120 mmHg. His peripheral circulation is compromised. Mr Jones had an ankle duplex test to evaluate the extent of his peripheral vascular disease. The results of the ankle brachial index: decreased on the left (0.60) compared to the right (0.95) NR>0.9. There was a significant drop in ABI on treadmill exercise testing in the left leg and a mild fall in the right leg. The exercise test was terminated after one minute because of severe left calf pain. Left peripheral arterial scan demonstrated an occluded left superficial femoral artery with collateral flow into a patent popliteal artery. Six months following the initial consultation Mr Jones presents for follow-up. He has stopped smoking and has reduced his alcohol intake. He has been very strict with his diet and managed to lose 12 kg of weight. His hypertension, diabetes and hyperlipidaemia are now well controlled. His claudication distance is unchanged, if anything slightly worse. He would like to be able to exercise more and is keen to have his peripheral circulation improved.
5. What investigation will be required prior to any intervention? What are the risks that are involved with this investigation?
Suggested Time = 5 min Question 5 of 7 Cumulative Time = 102 min
Six months following the initial consultation Mr Jones presents for follow-up. He has stopped smoking and has reduced his alcohol intake to 20 grams a day. He has been very strict with his diet and managed to lose 12 kg of weight. He is normotensive on an ACE inhibitor. His random blood sugar level is 7 mmol/L (NR 3.0-7.7mmol/L) and his fasting lipids are much improved with diet and statin medication. His claudicant distance is unchanged, if anything slightly worse. He would like to be able to exercise more and is keen to have his peripheral circulation improved. Andrew mentions that he was recently reading a magazine article that suggested medical science had ‘conquered’ heart disease toward the end of the twentieth century.
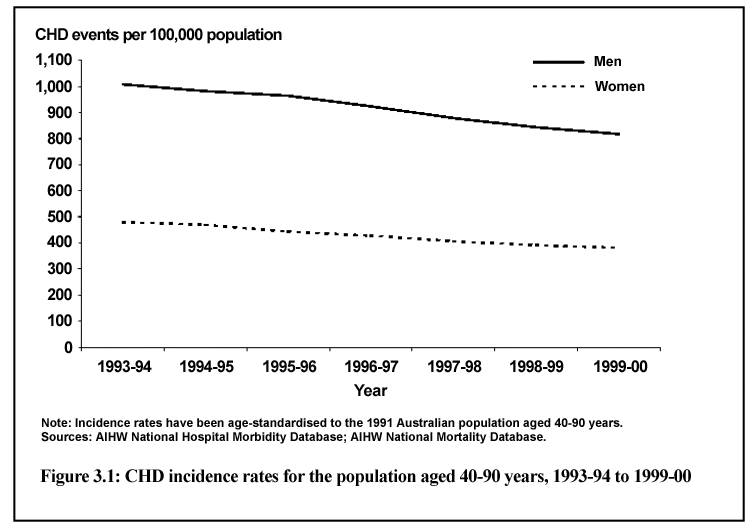
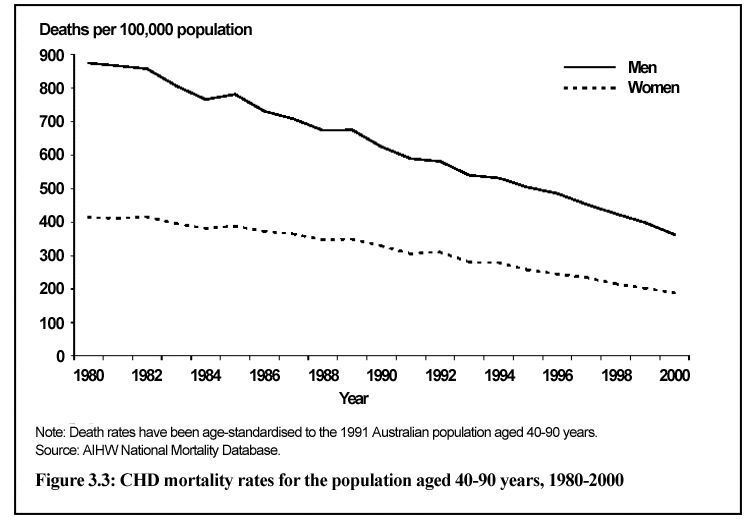
6. Using the graphs opposite, identify THREE trends you would use to respond to Andrew with respect to coronary heart disease (CHD) in Australia in recent years.
Suggested Time = 7 min Question 6 of 7 Cumulative Time = 109 min
The following graph comes from the “Epidemic of coronary heart disease in Australia and its treatment” Sept 2002 AIHW.
Six months following the initial consultation Mr Jones presents for follow-up. He has stopped smoking and has reduced his alcohol intake to 20 grams a day. He has been very strict with his diet and managed to lose 12 kg of weight. He is normotensive on an ACE inhibitor. His random blood sugar level is 7 mmol/L (NR 3.0-7.7mmol/L) and his fasting lipids are much improved with diet and statin medication. His claudicant distance is unchanged, if anything slightly worse. He would like to be able to exercise more and is keen to have his peripheral circulation improved. Andrew mentions that he was recently reading a magazine article that suggested medical science had ‘conquered’ heart disease toward the end of the twentieth century.
7. List one primary, one secondary and one tertiary prevention strategy that might have contributed to the reduction of mortality rates of coronary heart disease in the last twenty years.
Suggested Time = 6 min Question 7 of 7 Cumulative Time = 115 min
END OF CASE 3
Jill Townsend, aged 17 years, presents to the Emergency Department with a 3 day history of increasing cough, wheeze and breathlessness. She has a history of asthma since the age of 5 years with 4 previous admissions to hospital in the last 2 years.
1. Which clinical signs would you look for to help you assess the severity of Jill’s acute asthma?
Suggested Time = 5 min Question 1 of 7 Cumulative Time = 120 min
Jill Townsend, aged 17 years, presents to the Emergency Department with a 3 day history of increasing cough, wheeze and breathlessness. She has a history of asthma since the age of 5 years with 4 previous admissions to hospital in the last 2 years. Jill has symptoms of a viral upper respiratory tract infection. She is breathless and using her accessory muscles. There are moderately loud wheezes heard over both lungs. 2. What investigations will you organize for Jill? Justify each of your choices.
Suggested Time = 5 min Question 2 of 7 Cumulative Time = 125 min
Jill Townsend, aged 17 years, presents to the Emergency Department with a 3 day history of increasing cough, wheeze and breathlessness. She has a history of asthma since the age of 5 years with 4 previous admissions to hospital in the last 2 years. Jill has symptoms of a viral upper respiratory tract infection. She is breathless and using her accessory muscles. There are moderately loud wheezes heard over both lungs. Jill has an FEV1 of 50% of the predicted value. Her oxygen saturation is 88% (NR 95-98%).
3. Describe your immediate management plan. 4. Justify each of your management decisions.
Suggested Time = 8 min Questions 3 & 4 of 7 Cumulative Time = 133 min
Jill Townsend, aged 17 years, presents to the Emergency Department with a 3 day history of increasing cough, wheeze and breathlessness. She has a history of asthma since the age of 5 years with 4 previous admissions to hospital in the last 2 years. On examination she is breathless and moderately loud wheezes are heard over both lungs. She has an FEV1 of 50% of the predicted value. Her oxygen saturation is 88% (NR 95-98%). Jill was admitted to the ward and treated with oxygen, oral prednisone and nebulised salbutamol. Prior to admission Jill had been on fluticasone 100 ug bd and a salbutamol inhaler prn (used at least 4 x daily). By noon of the following day Jill is much better. Her PFR is 80% of predicted, the FEV1 is 70% of predicted and oximetry shows 95% saturation. You decide that she is ready to be discharged. 5. What management plan and advice will you provide to Jill?
Suggested Time = 5 min Question 5 of 7 Cumulative Time = 138 min
Jill Townsend, aged 17 years, presents to the Emergency Department with a 3 day history of increasing cough, wheeze and breathlessness. She has a history of asthma since the age of 5 years with 4 previous admissions to hospital in the last 2 years. Jill has an FEV1 of 50% of the predicted value. Her oxygen saturation is 88% (NR 95-98%). Jill was admitted to the ward and treated with oxygen, oral prednisone and nebulised salbutamol. Prior to admission Jill had been on fluticasone 100 ug bd and a salbutamol inhaler prn (used at least 4 x daily). By noon of the following day her PFR is 80% of predicted, the FEV1 is 70% of predicted and oximetry shows 95% saturation. You decide that she is ready to be discharged. Jill is reviewed by her local doctor who commences her on a single inhaler device which delivers both an inhaled corticosteroid plus a long acting beta adrenoceptor agonist. 6. Describe the cellular and/or molecular mechanisms that provide a rational basis for use of a combination of inhaled corticosteroid plus a long acting beta adrenoceptor agonist.
Suggested Time = 6 min Question 6 of 7 Cumulative Time = 144 min
Jill Townsend, aged 17 years, presents to the Emergency Department with a 3-day history of increasing cough, wheeze and breathlessness. She has a history of asthma since the age of 5 years with 4 previous admissions to hospital in the last 2 years. Jill has symptoms of a viral URTI and has an FEV1 of 50% of the predicted value. Her oxygen saturation is 88% (NR 95-98%). Jill was admitted to the ward and treated with oxygen, oral prednisone and nebulised salbutamol. Prior to admission Jill had been on fluticasone 100 ug bd and a salbutamol inhaler prn (used at least 4 x daily). By noon of the following day Jill is much better and ready for discharge. She is reviewed by her local doctor who commences her on a single inhaler device which delivers both an inhaled corticosteroid plus a long acting beta adrenoceptor agonist. Asthma is one of Australia’s National Health Priority areas and affects over two million (11%) Australians. The National Asthma Action Plan 1999-2002 is an important Commonwealth government strategy aimed at improving the quality of life and health outcomes of people with asthma, reducing the social and economic impact of asthma, optimizing the clinical management and reducing the prevalence, incidence and severity of asthma in the Australian community. One of the key components of this strategy is consumer education. 7. List 4 key content areas of patient education that should be reviewed with Jill when she presented for general practice follow-up. Only your first 4 responses will be marked. Please number items.
Suggested Time = 6 min Question 7 of 7 Cumulative Time = 150 min
Biblical Herbs as Alternatives to Pharmaceuticals ??? James Duke, PhD No one really knows whether these are as good (or as bad) as the pharmaceuticals until they have been clinically compared. The herbal alternatives need to be clinically compared, especially since nearly 25% of North Americans cannot afford the pharmaceutical prescription and/or the doctor to prescribe them. I recommend we suppo
Boa Noite meus senhores Cá estou eu novamente, Para deixar o meu testamento A esta humilde gente! Cá estou eu, O Judas falso e traidor Que só por trinta dinheiros Vendeu o Nosso Senhor! Entreguei-o aos judeus Mas não era isso que eu queria Iludi-me pelo dinheiro Que era uma ninharia. Mas vou pagar o mal que fiz, De tal acção ter praticado E não tardará muito tempo Que o fogo me seja lan
 The following graph comes from the “Epidemic of coronary heart disease in Australia and its treatment” Sept 2002 AIHW.
Six months following the initial consultation Mr Jones presents for follow-up. He has stopped smoking and has reduced his alcohol intake to 20 grams a day. He has been very strict with his diet and managed to lose 12 kg of weight. He is normotensive on an ACE inhibitor. His random blood sugar level is 7 mmol/L (NR 3.0-7.7mmol/L) and his fasting lipids are much improved with diet and statin medication. His claudicant distance is unchanged, if anything slightly worse. He would like to be able to exercise more and is keen to have his peripheral circulation improved. Andrew mentions that he was recently reading a magazine article that suggested medical science had ‘conquered’ heart disease toward the end of the twentieth century.
The following graph comes from the “Epidemic of coronary heart disease in Australia and its treatment” Sept 2002 AIHW.
Six months following the initial consultation Mr Jones presents for follow-up. He has stopped smoking and has reduced his alcohol intake to 20 grams a day. He has been very strict with his diet and managed to lose 12 kg of weight. He is normotensive on an ACE inhibitor. His random blood sugar level is 7 mmol/L (NR 3.0-7.7mmol/L) and his fasting lipids are much improved with diet and statin medication. His claudicant distance is unchanged, if anything slightly worse. He would like to be able to exercise more and is keen to have his peripheral circulation improved. Andrew mentions that he was recently reading a magazine article that suggested medical science had ‘conquered’ heart disease toward the end of the twentieth century.