Tadalafil entfaltet seine Wirkung über eine selektive Hemmung der PDE5, wodurch die Konzentration von cGMP im glatten Muskelgewebe stabil bleibt. Diese biochemische Modulation resultiert in einer langanhaltenden Relaxation der Gefäßwände. Der Wirkstoff wird nach oraler Einnahme effizient resorbiert, mit einer Bioverfügbarkeit von rund 80 %. Seine Halbwertszeit von bis zu 36 Stunden ist innerhalb dieser Substanzklasse außergewöhnlich. Abgebaut wird er in der Leber, hauptsächlich durch CYP3A4, mit anschließender biliärer Exkretion. Typische unerwünschte Wirkungen entstehen durch eine verstärkte Vasodilatation, etwa Kopfschmerzen oder Flush. Pharmakologisch wird cialis generika vor allem durch die verlängerte Wirkungsdauer charakterisiert.
Mamazone.de
Breast Cancer Research and Treatment 61: 145–150, 2000. 2000 Kluwer Academic Publishers. Printed in the Netherlands. Patients’ understanding of their own disease and survival potential in patients with metastatic breast cancer
Hitoshi Okamura1, Noboru Yamamoto2, Toru Watanabe2, Noriyuki Katsumata2, ShigemitsuTakashima3, Isamu Adachi2, Akira Kugaya1, Tatsuo Akechi4, and Yosuke Uchitomi11Psycho-Oncology Division, National Cancer Center Research Institute East; 2Department of Medical Oncology,National Cancer Center Hospital; 3Department of Surgery, National Shikoku Cancer Center Hospital; Chairmanof the Breast Cancer Study Group of the Japan Clinical Oncology Group (JCOG); 4Psychiatry Division, NationalCancer Center HospitalKey words: clinical trial, informed consent, metastatic breast cancer, survival, understanding
Purpose: To investigate the effect of understanding their own disease by patients with metastatic breast cancer ontheir survival potential after being informed by their physician. Patients and methods: Two hundred and fourteen women with metastatic breast cancer who participated in a
multi-institutional, randomized phase III trial (Japan Clinical Oncology Group (JCOG) Study 8808) were askedwhether they understood their own disease after being given information about the clinical trial. They were classi-fied into two groups on the basis of whether they understood or not. We estimated their survival after the time ofregistration and derived relative hazard ratios from Cox’s proportional hazards model. Results: There were 190 patients in the ‘better understanding’ group and 24 in the ‘poor understanding’ group.
Median survival times after registration were 28.3 and 16.1 months, respectively. The ‘better understanding’ groupshowed a significant difference from the ‘poor understanding’ group (p = 0.016). In multivariate regressionanalysis, patients who did not understand still showed poorer survival than those who understood (hazard ratio= 2.09; 95% confidence interval (CI) 1.16–3.78; p = 0.014). Conclusion: These results support the supposition that patients’ understanding of information about their
disease may influence their survival. Thus, it is important to evaluate patients’ recognition about informationeven after obtaining their consent. However, further investigation is needed to clarify the exact nature of thisrelationship. Introduction
Psycho-oncology research has shown that some
psychosocial and behavioral factors such as social sup-
Why is informed consent important for cancer pa-
port [6], coping strategies [7], and psychiatric group
tients? It has been emphasized that all cancer research
interventions [8, 9] can contribute to cancer patients’
demands fully informed consent from all patients [1–
quality of life or length of survival. Social or emotional
3], but an explicit answer to this question has not yet
support is thought to promote biological or behavi-
been provided. In randomized clinical trials, patients
oral adaptation in the face of stress [10] and result
should know about the potential randomization, all
in better compliance with treatment [11]. Richardson
the treatment options, and their own disease through
et al. [12] found that improving patient compliance
the information they are given. However, some reports
with treatment was associated with significant pro-
show that patients are not always given full informa-
longation of patient survival. Furthermore, support
tion [4] and that they do not always give their consent
from the physician is reported to be the most important
after they have understood the information [5].
source of support [13] and a significant predictor of
coping response [14]. This means that support from
age, marital status, Eastern Cooperative Oncology
the physician help patients cope better with cancer
Group performance status (PS), menopausal status,
[15]. Better support from the physician leads to an
disease-free interval (DFI), assigned therapy, recur-
attitude of fighting spirit in patients [7, 16] or active
rent or advanced disease, estrogen receptors (ER) and
behavioral coping [9], which is associated with bet-
progesterone receptors (PgR), axillary nodal status,
ter survival. Psychiatric interventions are suggested
history of adjuvant therapy, sites and number of meta-
to foster improved health habits such as better nu-
stases, blood counts, biochemical data, and serum tu-
trition and exercise regimens, and enhance effective
mor markers. Age, marital status, PS, and menopausal
and active behavioral coping, resulting in improved
status were determined at the time of registration. ER,
physician–patient relationships, positive mental atti-
PgR, and axillary nodal status were determined at
tudes, and greater compliance with treatment [12].
the time of primary diagnosis. Mean patient age at
However, no published data are available concerning
registration was 54.5 years (SD 9.7; range 24–72).
the relationship between informed consent and quality
We estimated the duration of survival from the time
of registration to either death or the date of the last
In this study, we tried to answer the initial question
from the viewpoint of psycho-oncology. We used datafrom a multi-institutional, prospective, randomized
phase III trial conducted by the Japan cooperative on-cology group (JCOG). Our objective was to investigate
The chi-square test, Fisher’s exact probability test, or
the effect of patients’ understanding of their disease
t-test was used for comparing the characteristics of
on their survival after being informed by their physi-
patients and tumors. Survival rates were calculated us-
cian. All the patients had metastatic breast cancer and
ing the Kaplan–Meier method [18]. All deaths were
counted, regardless of their cause. Each patient wasconsidered alive at the time of her last evaluationunless death had been documented. The stratified log-rank test was used for comparison of survival curves,
Patients and methods
and censored data were taken into account [19]. Bothunivariate and multivariate analyses were used for the
Women with metastatic breast cancer who particip-
analysis of potential prognostic factors. All factors
ated in a multi-institutional, randomized clinical trial
other than age were dichotomized and coded as 0
(JCOG study 8808) were studied. This trial consisted
(reference level) or 1. Age was evaluated as a continu-
of two therapy regimens to allow comparison of hor-
ous variable. For determination of the most significant
monal agents: ACT (doxorubicin, cyclophosphamide,
variables contributing to survival, the Cox propor-
tamoxifen) and ACM (doxorubicin, cyclophospham-
tional hazards model was applied [20]. Differences
ide, medroxyprogesterone) [17]. Patients were ran-
with a P value of less than 0.05 were considered
domly assigned to receive either of the regimens, and
significant. All P values were two-sided. Analyses
were recruited between December 1988 and Decem-
of prognostic factors in this patient population are
ber 1991; 218 patients agreed to participate. Patients
reported in detail elsewhere [21]. All data analyses
with severe mental disorders or cognitive impairment
used SPSS Version 6.1 statistical software (SPSS Inc.,
Before the initial treatment, the patients were asked
in writing ‘To what extent do you understand yourown disease after being informed by your physician
during the explanation of the clinical trial?’ Two hun-dred and fourteen women (98.2%) replied. Responses
Patients’ classification and characteristics
were graded 1 (understand well), 2 (understand tosome extent), 3 (understand only a little), 4 (do not
Ninety-five patients (44.4%) understood well, 95 un-
understand well), or 5 (do not understand at all). After
derstood to some extent, 18 (8.4%) understood only a
the first cycle of treatment, we asked the question
little, 3 (1.4%) did not understand well, and 3 did not
understand at all. Their median survival times were
For all patients, with permission of the JCOG data
28.3, 28.5, 20.9, 10.5 and 10.0 months, respectively.
center, we gathered data from case report forms on
From this result, we thought it was appropriate to
Patients’ understanding and survival potentialTable 1. Distribution of selected characteristics in patients among ‘better under-standing’ group and ‘poor understanding’ group
∗Chi-square test, Fisher’s exact probability test, or t-test (age). Table 2. Comparison os survival classified into two groups according to their understanding of their disease: ‘betterunderstanding group’ and ‘poor understanding group’
Abbreviation: MST, median survival time.
consider patients in the first two groups together, andcompare them with the patients in the last three groupscombined. Therefore, 190 patients (89%) formed the‘better understanding’ group and 24 patients (11%)formed the ‘poor understanding’ group.
Table 1 summarizes the characteristics of patients
and tumors. There were no significant differences inany factors between the two groups. At the time ofanalysis, the median follow-up time was 25.5 months(range 0.9–97.1). For the 30 censored patients stillalive, the median follow-up time was 79.9 months
Figure 1. Comparative survival curves of patients classified accord-
ing to their understanding of their disease: ‘better understanding’group and ‘poor understanding’ group. P values were calculated by
Follow-up data regarding patients’ understanding
When the question was repeated after the first cycle of
(p = 0.033), serum aspartate aminotransferase (AST)
treatment, only 10 patients (4.6%) gave answers that
(p < 0.01), serum alanine aminotransferase (ALT)
were different to those before treatment: four from
(p < 0.01), serum alkaline phosphatase (ALP) (p <
poor understanding to better understanding, and six
0.01), serum carcinoembryonic antigen (CEA) (p =
from better understanding to poor understanding.
0.02), and serum CA15-3 (p < 0.01), as well as pa-tient understanding. Based on these significant factors
Comparison of survival between the two groups
and on adjuvant chemotherapy, which is an important
Table 2 lists survival rates from 1 to 5 years and
prognostic factor for patients with metastatic breast
the median survival times. The median survival times
cancer, multivariate regression analyses using the Cox
were 28.3 months for the ‘better understanding’ group
proportional hazard model were conducted to identify
(95% CI 22.3–34.3), and 16.1 months for the ‘poor
factors that independently had the most important
understanding’ group (95% CI, 8.1–24.0). The ‘poor
prognostic influence on survival. Stepwise regression
understanding’ group also showed a significantly dif-
procedures were applied to calculate the values of the
ferent overall survival from the ‘better understanding’
beta-coefficients of the Cox model. After adjustment
group (p = 0.016) (Figure 1).
for age, which is suggested to be associated with pa-tients’ understanding, patients who did not understand
Univariate and multivariate analyses
still had poorer survival than those who understood(hazard ratio = 2.09; 95% CI, 1.16–3.78; p = 0.014)
Univariate analysis of pretreatment characteristics of
patients and tumors revealed significant prognostic in-fluences for DFI (p < 0.01), PS (p < 0.01), distantlymph nodes metastasis (p = 0.032), liver metastasis
Discussion (p < 0.01), number of metastatic sites (p = 0.029),hemoglobin (Hb) (p = 0.025), serum lactic dehyd-
Informed consent is the basic component of all cancer
rogenase (LDH) (p < 0.01), serum total protein (TP)
care and is considered an essential psychosocial, be-
Patients’ understanding and survival potentialTable 3. Multivaliate survival analysis using Cox’s proportional hazard model
∗The lower range of each category is the reference category.
havioral, and ethical aspect of cancer treatment. The
the hospital, resulting in greater treatment compli-
present study showed that patients who reported that
ance. However, treatment compliance with the clinical
they did not understand their disease after being in-
trial was not apparent in this study. The relative dose
formed by their physician during the explanation of
intensity of doxorubicin (intravenous) was approxim-
the clinical trial had poorer survival than patients who
ately 90% in both treatment arms, and the patients
reported that they understood. As there were no dif-
were asked at each clinic visit whether they had swal-
ferences in medical factors between the two groups
lowed the prescribed drugs. However, no records were
classified according to patients’ understanding, some
available. Therefore, although these explanations are
other factor such as psychosocial or behavioral factor
still highly speculative and further studies are needed,
might have contributed to their survival.
our findings support the supposition that it is import-
Considering the previous reports on the relation-
ant to evaluate patients’ understanding of information,
ship between psychosocial or behavioral factors and
even after their consent has been obtained.
survival, there are a number of possible reasons why
The major limitations of this study were the use
patients who do not understand their disease have
of only a single item for measuring patients’ under-
higher mortality from cancer. One possibility is related
standing of their disease and the lack of measurement
to social support from physicians [7, 9, 16]. Patients
of other variables that might have helped to explain
who do not understand their disease may not be able
the link between understanding and survival. It is un-
to talk honestly with their physician in order to solve
clear why 24 patients (11%) reported that they did not
problems, develop an attitude of partnership with the
understand their disease, although they were all able
physician, and consequently receive better support.
to read, speak, and communicate in Japanese. It is
Another possibility is related to patients’ coping or
unlikely that these patients were unable to understand
behavior [7, 12]. Understanding the nature and course
due to mental problems, because the eligibility cri-
of the disease may change patients’ behavior, that is,
teria for this clinical trial excluded patients with severe
patients who understand their disease may acquire bet-
mental disorders or cognitive impairment. Education
ter health habits and self-care and regularly consult
level, which was not evaluated in this study, may be
an important factor in explaining the reason for differ-
Fawzy FI, Fawzy NW, Hyun CS, Elashoff R, Guthrie D,
ences in patients’ understanding of their disease [22,
Fahey JL, Morton DL: Malignant melanoma. Effects of anearly structured psychiatric intervention, coping, and affect-
23]. However, there were no illiterate patients, among
ive state on recurrence and survival 6 years later. Arch Gen
whom the survival rate was reported to be lower than
that among patients who had more than 12 years of
House JS, Landis KR, Umberson D: Social relationships and
education [24]. It is possible that the patients may not
Spiegel D: Psychosocial intervention in cancer. J Natl Cancer
have wanted to understand the bad news. Furthermore,
the patients may not have understood on only one oc-
Richardson JL, Shelton DR, Krailo M, Levine AM: The ef-
casion, or sufficient information may not have been
fect of compliance with treatment on survival among patients
with hematologic malignancies. J Clin Oncol 8: 356–364,1990
In conclusion, this study had some limitations due
Slevin ML, Nichols SE, Downer SM, Wilson P, Lister TA,
to the retrospective analysis employed. However, it
Arnott S, et al.: Emotional support for cancer patients:
seems that the present results include important find-
What do patients really want? Br J Cancer 74: 1275–1279,
ings regarding the relationship between patients’ un-
Bloom JR: Social support, accommodation to stress and
derstanding of their disease after giving their informed
adjustment to breast cancer. Soc Sci Med 16: 1329–1338,
consent and length of survival. Therefore, it would be
worthwhile to investigate this relationship further.
Akechi T, Okamura H, Yamawaki S, Uchitomi: Predictorsof patients’ mental adjustment to cancer: patient charac-teristics and social support. Br J Cancer 77: 2381–2385,1998
Acknowledgements
Watson M, Greer S, Young J, Inayat Q, Burgess C, RobertsonB: Development of a questionnaire measure of adjustment to
We thank Ms. Ryoko Katayama, at the Psycho-
cancer: the MAC scale. Psychol Med 203–209, 1988
Watanabe T, Adachi I, Tajima K, Aoyama H, Sano M,
Oncology Division, National Cancer Center Research
Nomura Y: Improving the quality of life during chemoen-
Institute East, Japan, for her research assistance. This
docrine therapy for metastatic breast cancer: A randomized
study was supported in part by a grant-in-aid for
comparison of tamoxifen (TAM) versus medroxyprogesteroneacetate (MPA) in combination with doxorubicin (ADM) plus
cancer research and the second-term comprehensive
cyclophosphamide (CPA) (Abstract). Proc Am Soc Clin Oncol
10-year strategy for cancer control from the ministry
Kaplan EL, Meier P: Nonparametric estimation from incom-plete observation. J Am Stat Assoc 53: 457-481, 1958
Mantel N: Evaluation of survival data and two new rank orderstatistics arising in its consideration. Cancer Chemother Rep
References
Cox DR: Regression models and life-tables. J R Stat Soc B 34:
Meredith C, Symonds P, Webster L, Lamont D, Pyper E,
Gillis CR, Fallowfield L: Information needs of cancer patients
Yamamoto N, Watanabe T, Katsumata N, Omuro Y, Ando M,
in west Scotland: cross sectional survey of patients’ views.
Fukuda H, Tokue Y, Narabayashi M, Adachi I, Takashima S:
Construction and validation of a practical prognostic index
Meisel A, Kuczewski M: Legal and ethical myths about
for patients with metastatic breast cancer. J Clin Oncol 16:
Hopper KD, TenHave TR, Hartzel J: Informed consent forms
Appelbaum PS, Grisso T: Capacities of hospitalized, medic-
for clinical and research imaging procedures: how much
ally ill patients to consent to treatment. Psychosomatics 38:
do patients understand? Am J Roentgenol 164: 493–496,
Williams CJ, Zwitter M: Informed consent in European mul-
Sugarman J, McCrory DC, Hubal: Getting meaningful in-
ticentre randomised clinical trials – Are patients really in-
formed consent from older adults: a structured literature re-
formed? Eur J Cancer 30A: 907–910, 1994
view of empirical research. J Am Geriatr Soc 46: 517–524,
Wise J: Patients do not read consent forms. BMJ 313: 1421,
Gajalakshmi CK, Shanta V, Swaminathan R, Sankaranaray-
Maunsell E, Brisson J, Deschenes L: Social support and sur-
anan R, Black RJ: A population-based survival study on fe-
vival among women with breast cancer. Cancer 76: 631–637,
male breast cancer in Madras, India. Br J Cancer 75: 771–775,
Pettingale KW, Morris T, Greer S, Haybittle JL: Mental at-titudes to cancer: An additional prognostic factor. Lancet 1:
Address for offprints and correspondence:
Psycho-Oncology Division, National Cancer Center Research In-
Spiegel D, Bloom JR, Kraemer HC, Gottheil E: Effect of
psychosocial treatment on survival of patients with metastatic
Tel.: + 81-471-34-7013; Fax: + 81-471-34-7026; E-mail: yuchitom
Het afweersysteem is geprogrammeerd om elke verstoring te genezen op een voor ons minst schadelijke manier. Koorts, ten gevolge van een infectie is dus een noodzakelijke reactie voor genezing. Hetzelfde geldt voor snot en hoesten, omdat zij reinigende reacties van het lichaam zijn om bacteriën af te voeren. Ondersteun je afweersysteem met natuurlijke middelen en onderdruk je De winter is h
http://learnenglish.britishcouncil.org/en/magazine/food Introduction This support pack accompanies the video magazine article: Food . To read or listen to the article online, go to: This support pack contains the following materials: • a pre-watching vocabulary activity; • the article; • a comprehension task Before you read / listen Match the words and phrases in th
 Breast Cancer Research and Treatment 61: 145–150, 2000.
Breast Cancer Research and Treatment 61: 145–150, 2000.

 Patients’ understanding and survival potential
Table 1. Distribution of selected characteristics in patients among ‘better under-standing’ group and ‘poor understanding’ group
∗Chi-square test, Fisher’s exact probability test, or t-test (age).
Patients’ understanding and survival potential
Table 1. Distribution of selected characteristics in patients among ‘better under-standing’ group and ‘poor understanding’ group
∗Chi-square test, Fisher’s exact probability test, or t-test (age).




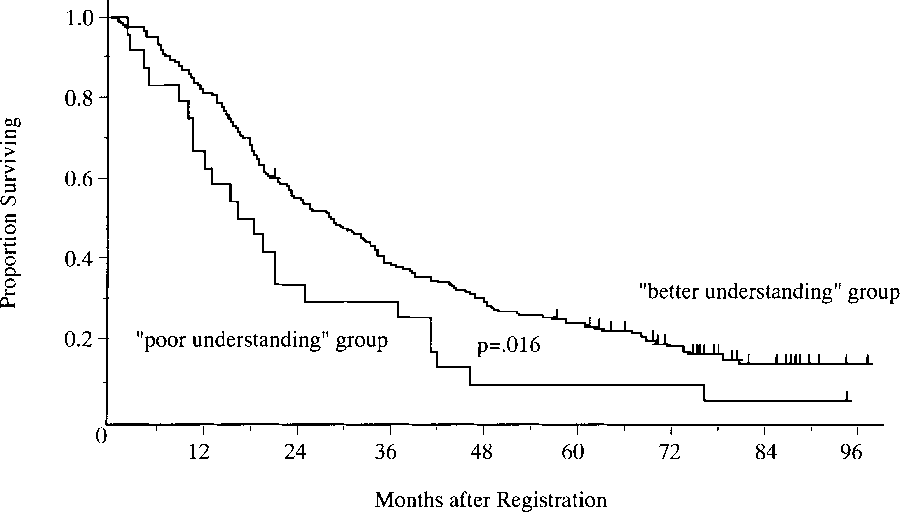 Table 2. Comparison os survival classified into two groups according to their understanding of their disease: ‘betterunderstanding group’ and ‘poor understanding group’
Abbreviation: MST, median survival time.
Table 2. Comparison os survival classified into two groups according to their understanding of their disease: ‘betterunderstanding group’ and ‘poor understanding group’
Abbreviation: MST, median survival time.

 Patients’ understanding and survival potential
Table 3. Multivaliate survival analysis using Cox’s proportional hazard model
∗The lower range of each category is the reference category.
Patients’ understanding and survival potential
Table 3. Multivaliate survival analysis using Cox’s proportional hazard model
∗The lower range of each category is the reference category.