Tadalafil entfaltet seine Wirkung über eine selektive Hemmung der PDE5, wodurch die Konzentration von cGMP im glatten Muskelgewebe stabil bleibt. Diese biochemische Modulation resultiert in einer langanhaltenden Relaxation der Gefäßwände. Der Wirkstoff wird nach oraler Einnahme effizient resorbiert, mit einer Bioverfügbarkeit von rund 80 %. Seine Halbwertszeit von bis zu 36 Stunden ist innerhalb dieser Substanzklasse außergewöhnlich. Abgebaut wird er in der Leber, hauptsächlich durch CYP3A4, mit anschließender biliärer Exkretion. Typische unerwünschte Wirkungen entstehen durch eine verstärkte Vasodilatation, etwa Kopfschmerzen oder Flush. Pharmakologisch wird cialis generika vor allem durch die verlängerte Wirkungsdauer charakterisiert.
Ultraviolet a1 phototherapy: a british photodermatology group workshop report
Ultraviolet A1 phototherapy: a British Photodermatology Groupworkshop report
A. C. Kerr, J. Ferguson, S. K. Attili, P. E. Beattie,* A. J. Coleman,† R. S. Dawe, B. Eberlein,‡V. Goulden,§ S. H. Ibbotson, H. du P. Menage,– H. Moseley, L. Novakovic,– S. L. Walker,–J. A. Woods, A. R. Young– and R. P. E. Sarkany–
Photobiology Unit, Ninewells Hospital, Dundee, UK; *Western Infirmary, Alan Lyell Centre for Dermatology, Glasgow, UK; †Medical Physics Department, Guy’sand St Thomas’ Hospital, London, UK; ‡Department of Environmental Dermatology and Allergology, Technische Universita¨t Mu¨nchen, Munich, Germany;§Department of Dermatology, Leeds General Infirmary, Leeds, UK; and –Photodermatology Unit, St John’s Institute of Dermatology, Guy’s and St Thomas’Hospital, London, UK
Whole-body ultraviolet (UV)A1 (340–400 nm) phototherapy was first introduced
30 years ago, but is currently available in the UK in only three dermatologydepartments. A workshop to discuss UVA1 was held by the British PhotodermatologyGroup in May 2009, the aim of which was to provide an overview of UVA1phototherapy and its role in practice, and to identify areas in which further studies arerequired. The conclusions were that UVA1 phototherapy is an effective treatment inseveral inflammatory skin diseases, including localized scleroderma and atopic eczema(AE); however, deficiencies and limitations exist in the published evidence base. Formost diseases, such as AE, other treatments also exist, which are generally moreeffective than UVA1. However, for some diseases, particularly morphoea, the evidenceof efficacy is stronger for UVA1 than for other treatments. Acute adverse effects ofUVA1 are minimal. The risk of long-term adverse effects, particularly skin cancer, isunknown. Medium to high doses of UVA1 are needed for efficacy in most situations,but the equipment to deliver such doses is large, expensive and difficult to install. UVA1is currently underprovided, and the recommendation of the workshop is that moretertiary centres should have access to UVA1 phototherapy in the UK.
answer several questions asked by clinicians: ‘Should I
be using UVA1 phototherapy?’; ‘Which patients benefit
Long-wavelength ultraviolet A (UVA1) (Fig. 1) was first
from UVA1 phototherapy?; and ‘Is UVA1 phototherapy
reported as a skin disease treatment in 1981.1 Thirty
years later, the published evidence on how best to use itremains limited and of variable quality.
A workshop to discuss UVA1 was held by the British
Photodermatology Group in May 2009, which aimed to
Dermatologists, physicists and scientists with experienceof or an interest in UVA1 were invited. All but one (BE,from Munich) were based in the three UVA1 centres in
Correspondence: Dr Alastair C. Kerr, Photobiology Unit, Department of
the UK. Each participant at the workshop reviewed an
Dermatology, Ninewells Hospital, Dundee DD1 9SY, UK
allocated area of therapy, and presented this to the group.
The literature review methods were not standardized, but
Conflict of interest: none declared.
levels of evidence were based on the Scottish Intercolle-
giate Guidelines (SIGN) system (see Appendix 1).
Ó The Author(s)CED Ó 2012 British Association of Dermatologists • Clinical and Experimental Dermatology, 37, 219–226
BPG UVA1 workshop report • A. C. Kerr et al.
diseases are summarized in Table 1. There have been
reviews of UVA1 disease indications,10 and specificallyfor fibrosing diseases such as morphoea.9,11 Most publi-cations describe UVA1 in terms of low, medium or highdose; these doses describe individual treatments rather
than cumulative dose over a course. Low doses can bedelivered using low-output, fluorescent lamp equipment,
whereas medium and high doses require larger and moreexpensive metal-halide lamp equipment. There are no
internationally agreed definitions of different treatment
doses but < 10 J ⁄ cm2 is generally considered ‘very lowdose’, 10–29 J ⁄ cm2 ‘low dose’, 30–59 J ⁄ cm2 ‘medium
Figure 1 The electromagnetic spectrum, illustrating the relative
dose’ and > 60 J ⁄ cm2 ‘high dose’.
position of UVA1 (340–400 nm) radiation.
Discussion at the workshop highlighted relevant publi-cations. Because the published studies on UVA1 remain
limited in number, much of the workshop outcome was
UVA1, at least at medium to high doses, is effective,
but has not been shown to be more effective than thestandard phototherapies (narrowband UVB12,13 and
psoralen UVA14) for atopic eczema (AE). In many of
UVA1 is different from other UV phototherapies because
the studies, UVA1 was used as monotherapy, rather
it penetrates deeper and has some different biological
than an adjunct to other standard therapies, which
effects. The cellular effects of UVA1 have more in
may limit extrapolation to clinical practice. UVA1 has
common with visible light than with UVA2 (320–
been found to be more effective than comparators in
‘acute eczema’15–20 and not more effective than
The key molecules that absorb UVA1 radiation,
leading to the biological effects, have not been conclu-
However, there has been no direct comparison of
sively identified. UVA1 mainly exerts its effects via
efficacy of UVA1 in ‘acute’ vs. ‘chronic’ eczema, so it is
unclear whether UVA1 has a specific role in the
absorption by endogenous photodynamic photosensitiz-
treatment of acute eczema. The workshop view was
ers including lipids and proteins.3,4 There is also recent
that UVA1 is valuable for some patients with AE
evidence that DNA can directly absorb UVA1 to form
unresponsive to other phototherapies; however, these
cyclobutane pyrimidine dimers.5 The effects of UVA1-
are few, and for most centres, the expense of high-
output UVA1 apparatus solely for this indication would
likely to contribute to its efficacy in inflammatory
disease. The greater susceptibility of malignant T cellsto free-radical damage may explain the efficacy of UVA1in mycosis fungoides.6 Other immune cells such as
Langerhans cells and mast cells may also be affected by
UVA1 is definitely effective and valuable in the treat-
UVA1, with effects distinct from those induced by UVA2
ment of fibrotic skin conditions, for which it can induce
or UVB. UVA1-induced 1O2 and hydrogen peroxide
lengthy periods of remission, and for which other
modulate the activity of matrix metalloproteinases
therapeutic options are limited (Table 1).10,11,22 For
produced by fibroblasts. Collagenase mRNA is up-
localized morphoea, UVA1 is the only treatment with
regulated in morphoea fibroblasts after UVA irradia-
published controlled-study evidence of efficacy.23 The
tion,7,8 a mechanism that is thought to underlie the
workshop concluded that it was clear that UVA1 in
efficacy of UVA1 in sclerotic and fibrotic dermatoses.9
fibrosing conditions can be beneficial for patients ifdisease restricts joint or chest movement, and also in
What is known about the efficacy of UVA1 in
stopping or slowing widespread disease. A common
side-effect is local skin darkening, which may limit
The points taken into consideration in the workshop
its use, especially where the primary problem is
regarding the efficacy of UVA1 for treating various skin
CED Ó 2012 British Association of Dermatologists • Clinical and Experimental Dermatology, 37, 219–226
BPG UVA1 workshop report • A. C. Kerr et al.
Table 1 Diseases that may respond to UVA1 phototherapy.
effective than low doses. Canworsen appearance but improvefunction, e.g. joint movement. PUVAis considered a standard therapyand has not yet been directly comparedwith UVA1
on systemic and possibly alsodermatological features of disease
specimens seem to decrease. Notall reports have shown benefit. Maybe more useful for headaches andbone pain than for appearance of rash
more appropriate than UVA1(e.g. H1-and H2 antihistamines,leucotriene receptor antagonists,UVB and PUVA)
who have not responded to PUVA,but effect may be temporary
UVB for PLC). Position not clearfor PLEVA
CTCL, cutaneous T-cell lymphoma; GVHD, graft-versus-host disease; HS, hypereosinophillic syndrome; PLC, pityriasis lichenoides chronica;PLEVA, pityriasis lichenoides et varioliformis acuta; PRP, pityriasis rubra pilaris; PUVA, psoralen ultraviolet A; SLE, systemic lupuserythematosus; UV, ultraviolet.
Ó The Author(s)CED Ó 2012 British Association of Dermatologists • Clinical and Experimental Dermatology, 37, 219–226
BPG UVA1 workshop report • A. C. Kerr et al.
in the context of a clinical governance system, to ensure
appropriate and safe use and follow-up.
Skin pigmentation (tanning), which can persist formonths, is the commonest problem. Patients should be
warned that in morphoea, the lesions may be morenoticeable after treatment, because of hyperpigmenta-
tion. Erythema is rarely a problem, particularly if priortesting to ascertain the minimal erythema dose (MED)
UVA1 can be generated using fluorescent tubes or
has been performed. With high-output therapy, an
filtered metal halide lamps (for a list of suppliers, see
immediate asymptomatic erythema generally occurs,
Appendix 2). The Waldmann UV 7001KÒ (Herbert
lasting for about 2 h after treatment. As UVA1 can
Waldmann GmbH & Co., Vilingen-Schwenningen,
provoke polymorphic light eruption, initial exposure of a
Germany) whole body treatment unit equipped with
small test area can indicate whether whole-body expo-
40 PhilipsÒ TL 100 W ⁄ 10R UVA1 fluorescent lamps
sure is likely to induce an eruption. Uncommon acute
(Philips Electronics UK Ltd, Guilford, U.K.) delivers a
adverse effects include recrudescence of herpes simplex,
mean patient irradiance of 20 mW ⁄ cm2, and is suitable
cholinergic urticaria, and transient and reversible
for low-dose UVA1 therapy. Practical delivery of
medium and high doses requires the higher (approxi-
The workshop recommended the need for caution
mately 60 mW ⁄ cm2) irradiance of metal-halide units
with UVA1 and concomitant photoactive medications,
such as the Sellamed 3000Ò unit for localized exposures
given that most drug-induced photosensitivity is UVA-
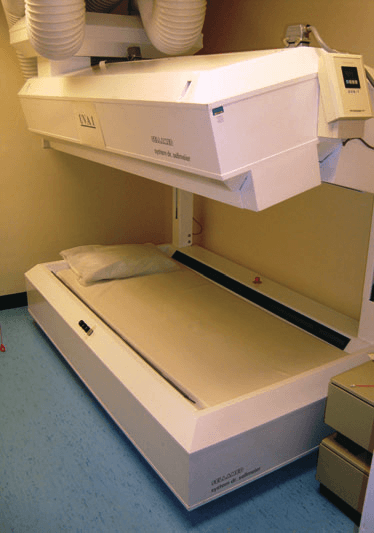
and the Sellamed 24000Ò bed (Sellas Medical Devices
dependent. Potential photosensitizers include fluoro-
GmbH, Gevelsburg, Germany) (Fig. 2) for whole-body
quinolone antibiotics and St John’s wort (hypericin).24Dietary psoralens have no significant effect.25 If apatient starts a photoactive drug during UVA1 treat-ment, the UVA1 MED should be rechecked. Thesuggested MED assessment dose ranges are 7–56 J ⁄ cm2for skin phototype I, 7–80 J ⁄ cm2 for phototype II, and10–112 J ⁄ cm2 for phototypes III and IV.
Studies of chronic UVA1 effects in humans are limited. Three retrospective studies involving 423 patients, whoreceived between 4 and 116 treatments in total,26–28reported no chronic effects. A case report of melanomaafter UVA1 and PUVA treatment has been published.29There is some limited information on UVA1 from animalmodels, showing that it can induce squamous cellcarcinomas and melanomas.
As with other phototherapies, there is no clearcutevidence on which to base a recommendation for amaximum lifetime number of treatments.30 Erring onthe side of caution, the workshop’s opinion was thatpatients receiving over 200 UVA1 whole body treat-ments should be considered at possibly being atincreased risk of skin cancer and managed accordingly.
Figure 2 The Sellamed 24000Ò bed for delivering ultraviolet A1
As with other phototherapies, UVA1 should be provided
CED Ó 2012 British Association of Dermatologists • Clinical and Experimental Dermatology, 37, 219–226
BPG UVA1 workshop report • A. C. Kerr et al.
treatment. Because of the heat-removal systems and
electrical cabling required, these high-dose sources areexpensive to install.
Over the past 15 years, it has become clear that UVA1phototherapy is a valuable treatment for some patients
Calibration ⁄ dosimetry ⁄ maintenance
with some uncommon and treatment-resistant skinconditions, and for a few patients with common condi-
The workshop advised performing UVA1 dosimetry
tions inadequately responsive to ‘standard’ photothera-
regularly, and one method was outlined. Firstly, the
pies. Although its mechanism of action is not yet fully
sensitivity factor of the meter should be established, and
understood, the formation of reactive oxygen species
the spectrum lamp measured using a calibrated spectro-
seems to be more important than the direct interaction of
radiometer. The integrated irradiance within the UVA1
UV with DNA. UVA1 is the first-line treatment for
range is then determined by spectroradiometry, and a
progressive morphoea or morphoea that is restricting
correction factor calculated. Secondly, the irradiance is
movement. Although effective in AE, UVA1 is best used
measured at different locations within the treatment
for cases in which other phototherapies have been
area; the average value over these locations then defines
inadequate. UVA1 therapy is generally well tolerated
the treatment irradiance. For a small source such as a
with few acute adverse effects, but the lack of long-term
300 · 300 mm field (e.g. Sellamed 3000Ò unit), 10
studies mean caution should be exercised because of the
locations may suffice, but a high-output Sellamed
possible increased risk of skin cancer and risk of photo-
24000Ò unit may need 30–40 locations measured. A
ageing. A number of different UVA1 devices are commer-
representative spectrum produced from the Sellamed
cially available. As with other phototherapies, accurate
maintenance and dosimetry is essential. Although somedata on UVA1 treatment regimens have been published,
Practical and financial issues around the use of
the evidence for these is often lacking.
ultraviolet A1 equipment in dermatology units
Crucial areas for future study are the establishment of
The main limitation on the availability of UVA1 in
the efficacy of UVA1 in different diseases, and identifica-
the UK and elsewhere is the cost and practical issues
tion of the minimum effective regimen for individual doses
associated with the machines. A high-output UVA1
and treatment courses. If lower individual treatment
device currently costs around £30 000, plus around
doses, even with the requirement for longer treatment
£10 000 for installation. Following installation, high
courses for a cumulative effect, are effective, this would
temperatures in the treatment room (requiring heat-
make UVA1 a practical and affordable option for
removal equipment) and long treatment times (limit-
more dermatology units, as treatment with medium and
ing the numbers of patients that can be treated) are
high individual doses requires expensive and bulky
issues that need consideration. Low-dose UVA1 using
equipment, thus restricting the availability of UVA1.
fluorescent sources is simpler to deliver and is cheaperto install, but more studies are required to discover
which patients can be effectively treated with low-doseUVA1.
• How does UVA1 phototherapy compare with more
readily available phototherapies, particularly PUVA,in the treatment of widespread morphoea?
• Is narrowband UVB or UVA1 most effective as an
adjunctive (to topical corticosteroid) therapy for
• Is the combination of UVA1 plus narrowband UVB
• Is UVA1 appropriate as an adjunctive therapy for
cutaneous lupus erythematosus, or should it be
Irradiance (W/cm 0.0E+00330
reserved for systemic lupus erythematosus (SLE)?
Wavelength (nm)
• What is the minimum therapeutically effective dose,
and is irradiance (determining practicable individual
Figure 3 Example of output spectrum of Sellamed 24000Ò unit. Representative spectra at 650 mm from bottom of bed to top of
treatment doses) important for each disease in which
canopy. Detector at 250 mm from bottom of bed.
Ó The Author(s)CED Ó 2012 British Association of Dermatologists • Clinical and Experimental Dermatology, 37, 219–226
BPG UVA1 workshop report • A. C. Kerr et al.
9 Kroft EB, Berkhof NJ, van de Kerkhof PC et al. Ultraviolet
A phototherapy for sclerotic skin diseases: a systematic
review. J Am Acad Dermatol 2008; 59: 1017–30.
10 Dawe RS. Ultraviolet A1 phototherapy. Br J Dermatol
• UVA1 is not a new treatment, but its adop-
tion in phototherapy centres worldwide has been
11 Breuckmann F, Gambichler T, Altmeyer P et al. UVA ⁄
UVA1 phototherapy and PUVA photochemotherapy in
• UVA1 is effective for various diseases, and is the
connective tissue diseases and related disorders: a research
first-line phototherapy for some types of morphoea.
based review. BMC Dermatol 2004; 4: 11.
• Some individual patients with AE benefit from
12 Legat FJ, Hofer A, Brabek E et al. Narrowband UV-B vs
UVA1, but in practice, its role is as second- or
medium-dose UV-A1 phototherapy in chronic atopic
dermatitis. Arch Dermatol 2003; 139: 223–4.
• UVA1 is effective at very low doses to treat SLE.
13 Majoie IM, Oldhoff JM, van Weelden H et al. Nar-
• More pragmatic studies are needed, using UVA1
rowband ultraviolet B and medium-dose ultraviolet A1
as an adjunct to other standard treatments, but for
are equally effective in the treatment of moderate tosevere atopic dermatitis. J Am Acad Dermatol 2009;
most indications, medium to high treatment doses
14 Tzaneva S, Kittler H, Holzer G et al. 5-Methoxypsora-
• Delivery of medium and high doses of UVA1
len plus ultraviolet (UV) A is superior to medium-dose
requires expensive, bulky, heat-producing, high-
UVA1 in the treatment of severe atopic dermatitis: a
output equipment, which is likely to be the main
randomized crossover trial. Br J Dermatol 2010; 162:
reason for the slow adoption of UVA1.
15 Krutmann J, Diepgen TL, Luger TA et al. High-dose UVA1
therapy for atopic dermatitis. results of a multicenter trial. J Am Acad Dermatol 1998; 38: 589–93.
16 Krutmann J, Czech W, Diepgen T et al. High-dose UVA1
therapy in the treatment of patients with atopic dermati-
1 Mutzhas MF, Holzle E, Hofmann C et al. A new apparatus
tis. J Am Acad Dermatol 1992; 26: 225–30.
with high radiation energy between 320 and 460 nm:
17 von Kobyletzki G, Pieck C, Hoffmann K et al. Medium-
physical description and dermatological applications. J
dose UVA1 cold-light phototherapy in the treatment of
severe atopic dermatitis. J Am Acad Dermatol 1999; 41:
2 Edstrom DW, Porwit A, Ros AM. Effects on human skin of
repetitive ultraviolet-A1 (UVA1) irradiation and visible
18 Kowalzick L, Kleinheinz A, Weichenthal M et al. Low dose
light. Photodermatol Photoimmunol Photomed 2001; 17:
versus medium dose UV-A1 treatment in severe atopic
eczema. Acta Derm Venereol 1995; 75: 43–5.
3 Kielbassa C, Roza L, Epe B. Wavelength dependence of
19 Dittmar HC, Pflieger D, Schopf E et al. [UVA1 photo-
oxidative DNA damage induced by UV and visible light.
therapy. Pilot study of dose finding in acute exacer-
bated atopic dermatitis] (in German). Hautarzt 2001;
4 Ravanat JL, Douki T, Cadet J. Direct and indirect effects of
UV radiation on DNA and its components. J Photochem
20 Tzaneva S, Seeber A, Schwaiger M et al. High-dose versus
medium-dose UVA1 phototherapy for patients with severe
5 Mouret S, Philippe C, Gracia-Chantegrel J et al. UVA-
generalized atopic dermatitis. J Am Acad Dermatol 2001;
induced cyclobutane pyrimidine dimers in DNA: a direct
photochemical mechanism? Org Biomol Chem 2010; 8:
21 Jekler J, Larko O. Phototherapy for atopic dermatitis with
ultraviolet A (UVA), low-dose UVB and combined UVA
6 Yamauchi R, Morita A, Yasuda Y et al. Different suscep-
and UVB two paired-comparison studies. Photodermatol
tibility of malignant versus nonmalignant human T cells
Photoimmunol Photomed 1991; 8: 151–6.
toward ultraviolet A-1 radiation-induced apoptosis.
22 Kroft EB, van de Kerkhof PC, Gerritsen MJ et al. Period
J Invest Dermatol 2004; 122: 477–83.
of remission after treatment with UVA-1 in sclerodermic
7 Gruss C, Reed JA, Altmeyer P et al. Induction of interstitial
skin diseases. J Eur Acad Dermatol Venereol 2008; 22:
collagenase (MMP-1) by UVA-1 phototherapy in morphea
fibroblasts. Lancet 1997; 350: 1295–6.
23 Kreuter A, Hyun J, Stucker M et al. A randomized con-
8 Petersen MJ, Hansen C, Craig S. Ultraviolet A irra-
trolled study of low-dose UVA1, medium-dose UVA1, and
diation stimulates collagenase production in cultured
narrowband UVB phototherapy in the treatment of
human fibroblasts. J Invest Dermatol 1992; 99:
localized scleroderma. J Am Acad Dermatol 2006; 54:
CED Ó 2012 British Association of Dermatologists • Clinical and Experimental Dermatology, 37, 219–226
BPG UVA1 workshop report • A. C. Kerr et al.
24 Beattie PE, Dawe RS, Traynor NJ et al. Can St John’s wort
(hypericin) ingestion enhance the erythemal responseduring high-dose ultraviolet A1 therapy? Br J Dermatol
UK-based suppliers of equipment that can be used to
deliver ultraviolet A1 phototherapy.
25 Beattie PE, Wilkie MJ, Smith G et al. Can dietary furano-
coumarin ingestion enhance the erythemal response
during high-dose UVA1 therapy? J Am Acad Dermatol
26 Rombold S, Lobisch K, Katzer K et al. Efficacy of
UVA1 phototherapy in 230 patients with various skin
diseases. Photodermatol Photoimmunol Photomed 2008;
Medizinische Gerate GmbH(Germany) (http://www.sellas.de)
27 Tuchinda C, Kerr HA, Taylor CR et al. UVA1 photother-
apy for cutaneous diseases: an experience of 92 cases in
the United States. Photodermatol Photoimmunol Photomed
28 Jacobe HT, Cayce R, Nguyen J. UVA1 phototherapy is
effective in darker skin: a review of 101 patients ofFitzpatrick skin types I–V. Br J Dermatol 2008; 159:691–6.
29 Wallenfang K, Stadler R. [Association between UVA1
and PUVA bath therapy and development of malig-
nant melanoma] (in German). Hautarzt 2001; 52:705–7.
To show an understanding of UVA1 phototherapy,
30 Dawe RS. There are no ‘safe exposure limits’ for photo-
including mode of action, indications and adverse
therapy. Br J Dermatol 2010; 163: 209–10.
The strength of published evidence was graded accord-
A 30-year-old woman has been diagnosed with mor-
ing to a modified version of the ranking system adopted
phoea restricting movement at her shoulders and right
by the Scottish Intercollegiate Guidelines Network
elbow. She has heard of ultraviolet (UV)A1 photother-
apy and wants to know more about how it might workin her condition. Which of the following is likely to be
the most important mechanism of action of UVA1 intreating morphoea?
High-quality meta-analyses, systematic reviews of
RCTs, or RCTs with a very low risk of bias
Well-conducted meta-analyses, systematic reviews,
Meta-analyses, systematic reviews, or RCTs with a
d) Increased fibroblast matrix metalloproteinase activity
e) UVA1-generated production of singlet oxygen
High-quality systematic reviews of case control or
cohort or studies, high-quality case–control orcohort studies with a very low risk of confounding
or bias, and a high probability that the relation-ship is causal
A 24-year-old man of skin phototype III with a lifelong
Well-conducted case–control or cohort studies
history of atopic eczema (AE) attends with repeated
with a low risk of confounding or bias, and amoderate probability that the relationship is
flares of his eczema. His eczema has been severe over the
past 3 years, with poor control despite use of 200–
Case–control or cohort studies with a high risk of
300 g betamethasone dipropionate 0.05% ointment
confounding or bias, and a significant risk that the
weekly, along with emollients. After 1 week of clobeta-
sol propionate 0.05% ointment, his eczema has
Non-analytical studies, e.g. case reports, case series
improved, but it continues to affect him severely. Whichof the following treatments would be most appropriate?
Ó The Author(s)CED Ó 2012 British Association of Dermatologists • Clinical and Experimental Dermatology, 37, 219–226
BPG UVA1 workshop report • A. C. Kerr et al.
b) Broadband UVB phototherapyc) High-dose UVA1 phototherapy
A 35-year-old man with systemic lupus erythematosus
has heard of UVA1 and seeks more information about it.
e) Psoralen ultraviolet A photochemotherapy (PUVA)
Which of the following wavebands corresponds toUVA1 emission?
A 36-year-old woman is very distressed by the progres-
sive worsening, with new lesions developing, of a
symmetrical eruption of pale brown patches predomi-
nantly over the trunk. Based on the clinical presentationand histopathological findings of a skin biopsy, hercondition has been diagnosed as widespread morphoea.
Which of the following treatments would be most
This learning activity is freely available online at
https://www.wileyhealthlearning.com/ced.aspx.
a) Calcipotriol ointmentb) Narrowband UVB
• Read the article in print or online, paying particular
attention to the learning points and any author
• Reflect on the article• Register or login online at www.wileyhealthlearning.
com/ced.aspx and answer the CPD questions
A 43-year-old woman with extensive plaque psoriasis,
• Complete the required evaluation component of the
who has failed to respond to a variety of topical
treatments, attends the clinic seeking phototherapy. Which of the following phototherapies would be the
Once the test is passed, you will receive a certificate and
the learning activity can be added to your RCP CPD
b) Broadband UVBc) Narrowband UVBd) Oral PUVAe) UVA1
CED Ó 2012 British Association of Dermatologists • Clinical and Experimental Dermatology, 37, 219–226
Boulder County Nature Association Colorado Bird Observatory Allegra Collister Nature Preserve Bird banding report - Spring 2000 Although nets had been set up two weeks earlier (when severe winds destroyed one 12M net), banding didn't beginuntil May 1st. Many area birders were reporting low numbers of birds; and, ACNP was not an exception. It wastoo quiet. Our first effort of the
Riesgo poco frecuente pero probable en un legrado evacuador Por Ofelia de Lorenzo Viernes, 22 de febrero de 2013, a las 10:06El Juzgado de 1ª Instancia nº 20 de Madrid, desestimó, en su Sentencia de 5 de Febrero de 2013, la demandapresentada por una paciente frente a la facultativa que la atendió y el centro sanitario donde se llevó a cabo el actomédico, debido a la secuelas que
 BPG UVA1 workshop report • A. C. Kerr et al.
BPG UVA1 workshop report • A. C. Kerr et al.